The Coronavirus disease identified in 2019 (COVID-19) pandemic has taken the whole world by surprise. Strict social distancing, curfews, and infection control measures have been implemented to mitigate the devastating effects of the disease. These measures have made it difficult for families to contact and visit their loved ones while hospitalized, which may negatively affect patients’ well-being in the intensive care unit (ICU). Patient and family experience while in the ICU reflects the quality of care and services provided.1 Improving communication and trust between families and physicians is vital to improving overall family satisfaction.2 Family support has been shown to improve the patients’ inspiration and psychological behavior.3 Moreover, family visits may reduce the frequency of delirium and decrease anxiety in the ICU.4 Patient experience in the ICU is challenging to measure; however, widely used and validated tools are available to assess patient and family satisfaction and the fulfillment of their needs and expectations.1,5
Given the importance of family support and the value of maintaining communication during a pandemic crisis, we used a hybrid telephone and video conferencing model to connect our ICU patients with their families. This study aims to assess the satisfaction among non-COVID-19 ICU patients and their relatives with video conferencing (VC) as a method of communication during the curfew period.
METHODS
Study Design
This was a prospective observational study conducted at the intensive care units at King Fahad Medical City (KFMC) in Riyadh and King Fahad Hospital (KFH) in Madinah during the COVID-19 curfew period in Saudi Arabia between March and April 2020. The baseline characteristics, the video conferencing data, and the critically ill patient and family surveys were collected during the visiting restriction period between March and July 2020. During this period there was no visitor nor sitter allowed under any circumstances in the ICU. The local Institutional Review Boards of the two centers approved the study.
Subjects
Participants were consecutive COVID-19 negative adult (age ≥ 14 years) patients admitted to the ICUs at the participating centers during the visiting restriction period between March and July 2020. Consented patients with a length of stay in the ICU of more than 48 hours with at least one video conference conducted with their families were included. Exclusion criteria included airborne precaution requirements regardless of the indication, ICU length of stay of less than 48 hours, previously included re-admitted patients, and patients or representatives who couldn’t communicate via the video conferencing application.
The Hybrid Telephone and Video Conferencing Model
Besides the daytime Telephone calls to update the families during the curfew period at the participating centers, we added a 10-minute daily daytime video conferencing (VC) between the families and their patients during their ICU stay. The study coordinators arranged suitable times with the families in advance. At the time of VC, the bedside nurse or the study coordinator prepared the application and remained inside the room with the patient until the call ended. The video conferencing was conducted via a smart device utilizing a secured video conferencing application (Zoom Videos Communications, Inc., San Jose, CA, USA). We chose Zoom because no download is required to join meetings, and it is free, easy to use, and accessible on all smartphones, tablets, and computers. Also, Zoom has high-security features, making it suitable to use in healthcare settings. Zoom meetings were end-to-end encrypted and were not recorded. Any family member could join the encounter as long as the patient’s representative permitted. Daily compliance with the hybrid telephone and video conferencing model was monitored by the study coordinator. The conduct of the study was regularly monitored by our study monitoring team, which consisted of one study coordinator and two dedicated site investigators from each site.
Measurements
Patient and family surveys included single answer questions evaluating the satisfaction with video conferencing as a method of communication during the visiting restriction period. Additionally, patient and family surveys included open-ended questions to reflect on the experience, feedback, and address encountered difficulties. Both surveys were taken after at least one video conferencing session. Patients completed their surveys personally while an independent surveyor completed the family satisfaction survey via a telephone interview with the family representative. A second family satisfaction survey was obtained after the discharge, transfer, or death of the patient. The video conferencing data, including compliance, date, and duration, were recorded. We also obtained the baseline characteristics of patients, including their age, gender, date of admission to the ICU, diagnosis, comorbidities, and date of transfer or death. The demographical data of the families, including age, gender, relation to the patient, and level of education, were recorded.
Outcomes
The primary outcome was the general satisfaction of critically ill non-COVID-19 patients and their families with video conferencing (VC) as a mean of communication during the visiting restriction period. We also evaluated the factors associated with high general satisfaction among families.
Statistical Analysis
Baseline characteristics, responses to the patient and family surveys, and ICU outcomes were reported as frequency, median (interquartile range IQR), or mean ± standard deviation (SD). The family representatives’ satisfaction predictors were examined using the second survey data as the patient outcome variable was only available then. Non-parametric methods (Spearman’s correlation, Wilcoxon Rank Sum test, and Kruskal–Wallis test) were used for the unadjusted analysis as the primary outcome variable was not normally distributed. Multiple linear regression (MLR) with a backward elimination technique was used for the adjusted analysis. A significance level of 0.2 was required to stay in the MLR models. The backward elimination technique was used as it generates simple and easy-to-interpret models, reduces the multicollinearity issue, and lowers the chance of overfitting. All analyses were performed using R statistical software version 3.4.3 (R Foundation for Statistical Computing).
Institutional Review Board (IRB)
This study was approved by the IRB department at King Fahad Medical City, Saudi Arabia. The IRB registration number with King Abdulaziz City for Science and Technology (KACST), Kingdom of Saudi Arabia is “H-01-R-012”. The IRB registration number with Office for Human Research Protections/National Institutes of Health (OHRP/NIH), USA is “IRB00010471”. Approval Number Federal Wide Assurance NIH, USA is “FWA00018774”.
RESULTS
Baseline Characteristics of Patients
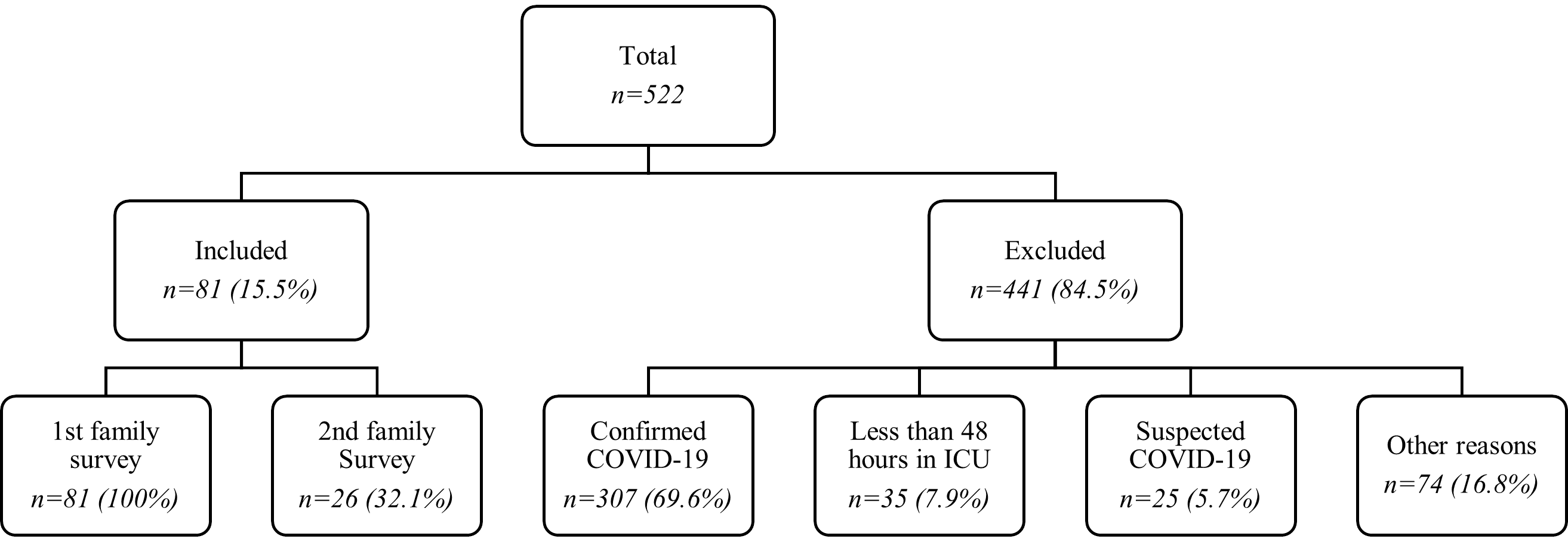
Of 522 screened patients, 81 (15.5%) met the inclusion criteria (Figure 1). The main reason for exclusion was active COVID-19 infection (69.6%). Baseline characteristics are shown in (Table 1). The mean age was 58.2 ± 19.2 years, and most patients were male (61.7%). The most frequent reason for admission was acute respiratory failure (25.9%) followed by septic shock (16.1%). The mean Charlson Comorbidity Index (CCI) was 3.8 ± 3.0, with diabetes and hypertension being the most frequently reported comorbidities (55.6% and 52.0%, respectively). The average Acute physiology and chronic health evaluation II (APACHE-II) score was 20.6 ± 6.8, and the ICU length of stay was 22.6 ± 17.9 days. Of 81 patients, 45 (56.3%) transferred to the floor, 23 (28.8%) passed away, 8 (10.0%) were discharged home, 4 (5.0%) transferred to a long-term facility, and one patient was still in the ICU at the end of the study data collection.

The Satisfaction of Critically Ill Non-COVID-19 Patients and Their Families with Video Conferencing
Of 81 family representatives initially surveyed, 26 (32.1%) family representatives underwent a follow-up survey (Figure 1). Around two-thirds of the family representatives were female (66.7%) with a mean age of 39.3 ± 11.8 (Table 1). Family representatives were mainly adult children (55.6%), followed by siblings (18.5%), partners (12.4%), and parents (6.2%) (Table 1). The patients’ median Glasgow Coma Scale (GCS) during the last VC before obtaining the first and second surveys were 10 (7, 13) and 11 (7, 13), respectively (Table 2). The average number of video conferencing conducted before obtaining the two surveys were 1 (1, 2) and 2 (1, 3), respectively (Table 2). The average duration of video conferencing was 9.7 ± 3.9 minutes.
During the first survey, most family representatives rated the effectiveness of the communication positively (87.7%), were satisfied with the VC timing (80.3%) and duration (70.4%), and preferred the VC method over the traditional one (71.6%) (Table 2). On a scale of 1-10, high general satisfaction was reported by family representatives in the initial survey (8.7 ± 1.7), with the majority reporting no visual, audio, or software difficulties. The second family survey revealed similar positive and satisfactory results (Table 2). Of 81 patients, 11 were included in the patient survey. On average, patients reported a high general satisfaction of 9.6 ± 0.7 with video conferencing, and all of them rated their experience positively.
Factors Associated with the General Satisfaction among Family Representatives
The association between the main variables of the second family survey and the general satisfaction was examined (Table 3). On unadjusted analysis, only the patients’ GCS at the time of VC was associated with the general satisfaction among family representatives (P=0.024) (Table 3). On adjusted analysis, higher patients’ Glasgow Coma Scale at the time of VC and increased number of VC sessions were associated with a higher family representatives’ satisfaction (P=0.001 and P=0.019, respectively) (Table 3).
DISCUSSION
This multicenter prospective observational study is the first to assess the satisfaction of adult critically ill non-COVID-19 patients and their families with video conferencing (VC) as a method of communication during the COVID-19 pandemic in Saudi Arabia. Our study demonstrated high general satisfaction with VC among patients and their family representatives. Most family representatives rated their experience with video conferencing positively and preferred it over traditional means of communication during the curfew.
Virtual communication to update families and replace family visits has been utilized before, mainly in the pediatric population.6–9 In 2011, Parsapour et al. reported their five years of experience with a video conferencing program to link patients with their families and friends when they cannot visit the hospital.6 The investigators concluded that video conferencing provides a practical solution to some barriers that may limit family presence.6 The feasibility of real-time video conferencing was also documented in another study in 2015 where parents of patients in the neonatal ICU received daily Skype or FaceTime updates.7 Similar to our results, most families perceived the intervention as meaningful, reliable, and easy to use.7 High satisfaction with the use of telemedicine was reported by remote parents who were unable to be present at their child’s bedside during the pediatric ICU rounds.8 Similar to our findings, most families reported that telemedicine encounters positively affected their level of reassurance regarding their patients’ care and improved communication with the care team.8
Increasing the ICU visiting hours can significantly decrease the incidence and length of delirium and length of ICU stay.10,11 However, it can interfere with patients’ care, increase the incidence of burnout among the ICU clinical staff, and lead to physical and emotional exhaustion of the families.12,13 Video conferencing, on the other hand, can provide the benefits of increasing visiting hours without its associated harm. Additionally, video conferencing serves as a great alternative to physical visits at times of curfews and visitation restrictions.
Besides being a great method for communication, video conferencing can also help improve the patient-and family-centred care approach.14
In our study, the general satisfaction among family representatives with video conferencing was not associated with the demographics of family representatives, length of ICU stay and patient’ outcome suggesting that the demonstrated high general satisfaction was a universal phenomenon across our cohort. As expected, higher patients’ GCS at the time of video conferencing and increased VC sessions were associated with higher family representatives’ satisfaction.
Our study has two main limitations. First, we excluded critically ill patients with COVID-19 as we prioritized the safety of our study staff. Despite this limitation, we believe that our study findings also apply to critically ill patients with COVID-19 as the demographics of the patients and their families are unlikely to be different during the study period merely based on the COVID-19 test result. The study was primarily conducted at the largest referral center in our country, making the study’s sample representative of a diverse group of patients and their families. Also, the high satisfaction with video conferencing among patients and their families was a universal finding in almost all the similarly designed studies conducted across various patient populations. Second, we only had patient survey data for 11 out of 81 patients. Reasons for missing data include patient death, patient low GCS, and incomplete patient survey. All the surveyed patients rated their experience with video conferencing positively and were generally highly satisfied with it. The high agreement among the surveyed patients will probably hold true for a larger group. Despite these limitations, we demonstrated that video conferencing is an effective and highly satisfactory method of communication between patients and their family representatives during curfews and visitation restrictions.
CONCLUSIONS
In summary, this multicenter observational study of a prospective cohort of non-COVID-19 critically ill patients shows that video conferencing is an effective mean of communication between patients and their families during the COVID-19 pandemic. It also demonstrates a high satisfaction with VC among patients and their family representatives regardless of their demographics, length of ICU stay and patient outcome. These findings provide strong evidence supporting the use of video conferencing to enhance the communication between patients and their families in different settings, including pandemic crises.
Acknowledgements
The authors would like to thank the Research Center at King Fahd Medical City, Riyadh, for their valuable financial support provided for the manuscript. We thank Yassmin A. Bukhari (King Fahad Medical City), Entsar Al Onazi and Kaouthar Sifaoui (King Fahad Hospital) for coordinating the video conferencing sessions and collecting the study data. We also thank Rahma F. Faraj, Maha T. Al Subaie, Fatma H. Alshehri and Reem M. Abdulhaq (King Fahad Medical City) for coordinating the video conferencing sessions and resolving their related issues. In addition. We thank Osama A. Nadhir for his help in drafting the initial manuscript.
Ethics statement
This study was approved by the Institutional Review Board (IRB) department at King Fahad Medical City, Saudi Arabia. The IRB registration number with King Abdulaziz City for Science and Technology (KACST), Kingdom of Saudi Arabia is “H-01-R-012”. The IRB registration number with Office for Human Research Protections/National Institutes of Health (OHRP/NIH), USA is “IRB00010471”. Approval Number Federal Wide Assurance NIH, USA is “FWA00018774”.
Data availability
The data used and/or analyzed in this study are not publicly available. However, data are available from the corresponding author upon reasonable request.
Funding
The study was not funded.
Authorship contributions
AHB collected data, performed simple analysis, interpreted data, drafting the study protocol and manuscript. MAG designed the study, performed statistical analysis, interpreted data, revised and edited the final manuscript. MSY, NSS created the surveys and collected the data from KFMC. HML revised the study protocol and edited the first manuscript. MAH, AMK collected and interpreted the data from KFH. MAM established and created the study idea, supervised the team. All authors reviewed the previous versions of the manuscript. All authors read and approved the final manuscript.
Disclosure of interest
The authors completed the ICMJE Disclosure of Interest Form (available upon request from the corresponding author) and disclosed no relevant interests.
Correspondence to:
Mohammed A Almaani
King Fahad Medical City, Riyadh Second Health Cluster
Prince Abdulaziz Ibn Jalwi St, P.O. Box: 59046, Riyadh 11525 Saudi Arabia
[email protected]