INTRODUCTION
Humanitarian crises caused by conflicts threaten access to health care, particularly in Africa. Countries in the Sahel region of Africa, such as Cameroon and Nigeria, face unprecedented humanitarian needs caused by armed conflict, poverty, climate change, food insecurity and political instability.1–3 The protracted humanitarian crises of the North West and South West regions of Cameroon and the North East states of Nigeria has led to the closure of 29% and 26% of the health facilities respectively, and the displacement of over 670,000 persons in Cameroon and 1.8 million persons in Nigeria.4–6 This has created a considerable gap in the availability and accessibility of health services to affected communities necessitating the increased use of different delivery models of care to bring health care to affected communities. Mobile clinics, community health workers and fixed care facility models are commonly used to provide primary health care (PHC) in humanitarian settings,7–10 which often present with complex and challenging operating environments. Under such circumstances, the humanitarian imperative to save lives, coupled with donor expectations and contextual realities,11 might motivate using one model over the other, though at the expense of quality.
To understand the factors that influence the use of the different models of care in conflict-affected settings, a mixed-method approach is necessary to enable researchers to map out current delivery models of care and understand the phenomena from the experiences, opinions and beliefs of humanitarian actors in selecting which model of care to use for service delivery.12,13 This article presents key methodological considerations that arose in a pilot qualitative study we conducted as part of a larger project titled “comparing primary health care delivery models in conflict settings of Cameroon and Nigeria”. The overall study uses a mixed-method sequential explanatory approach,12,14,15 beginning with a quantitative survey phase followed by a qualitative interview phase. The Consolidated Framework For Implementation Research (CFIR) was chosen as the framework to guide the analysis and reflections from this mixed methods study.16The pilot qualitative study was conducted after the first results from the cross-sectional survey were available. The survey results further shaped the questions and probes in the interview guides for the qualitative study. The interview guides were then pilot-tested before data collection for the qualitative part of the larger study.
Qualitative interviewing is an approach to obtain in-depth and rich information on specific areas of interest in their natural setting. In such inquiry, the researcher is key in the data collected, and the interview guide is the nucleus needed to obtain good qualitative data.17 Not only does having a carefully considered interview topic guide aid in systematically collecting accurate and robust qualitative data, it also allows consistency and comprehensiveness in the way the interviews are conducted.18 For qualitative studies involving more than one country, especially for research in conflict settings, developing and piloting the interview guides and methods to be used is good practice and important due to security challenges, cultural issues, and language barriers, which need to be considered to obtain good quality data.19 Researchers have suggested piloting interview guides to improve the researchers’ interviewing skills and refine questions to suit the setting and population group(s).20,21 Piloting refers to the initial study conducted to either validate the feasibility of the study or to pretest the instrument and procedures of the study.22 Considering our research is carried out in challenging operating environments (conflict-affected settings) involving communities who speak different languages, we piloted our interview instruments to ascertain safety and feasibility, learn from errors, refine the interview topic guides, and improve on interviewing skills. The researchers who collected data for the qualitative study had past experience in conducting interviews in stable environments but limited experience collecting quality qualitative data in fragile environments affected by conflict. The research team was made up of 5 women and 5 men. Data collection was led by a female PhD student, assisted by a male social science researcher and male medical doctor.
In this manuscript, we do not present findings from the pilot study but focus on the key methodological processes and lessons learnt from collecting qualitative data in conflict-affected countries with multiple languages.
THE METHOD (PROCESS)
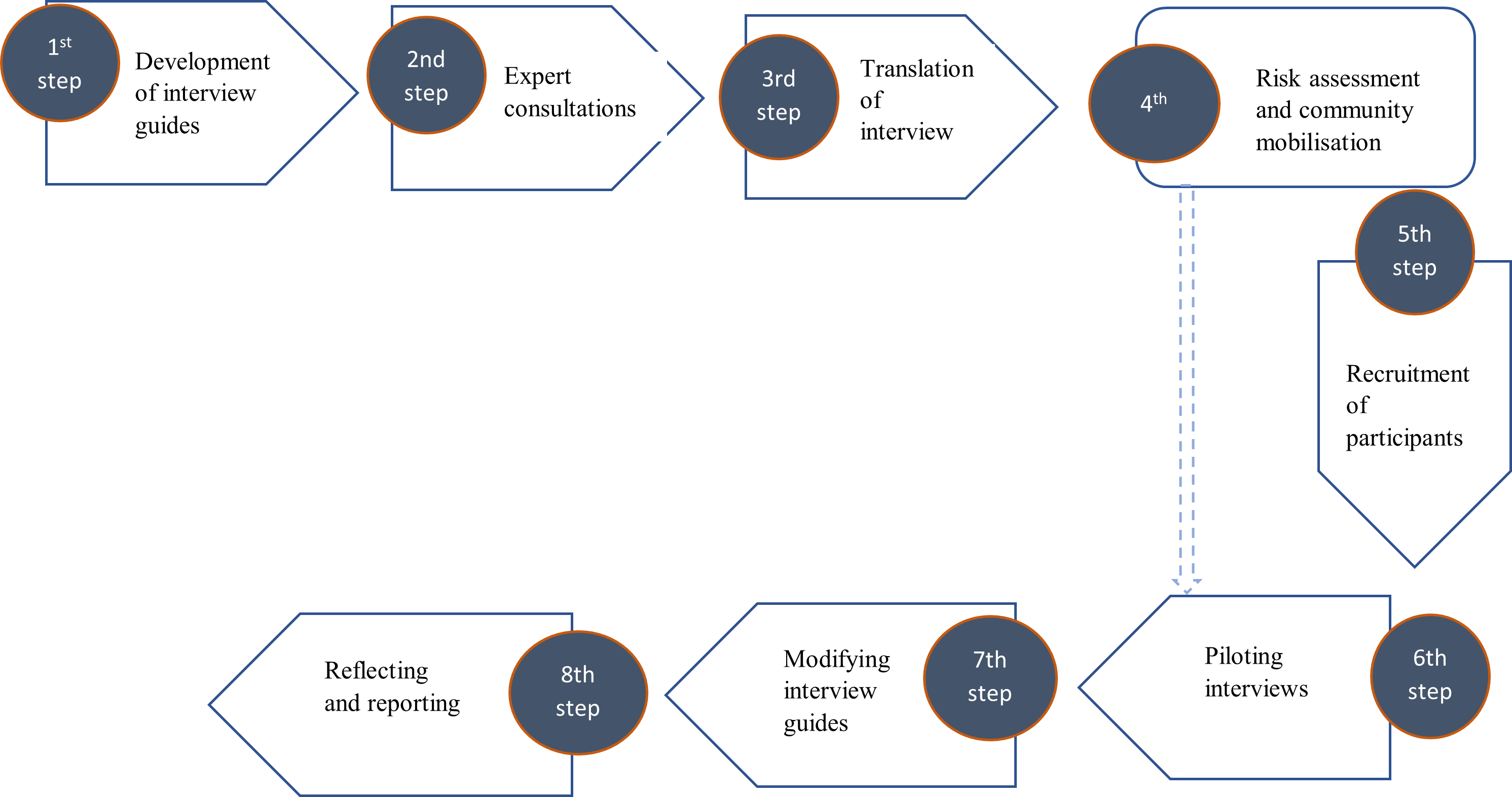
This article presents eight steps adopted by our team to pilot our interview protocols. In our adaptation process, we added two steps to previously suggested pathways.18,20,21,23 The steps included in our piloting process were: 1) development of interview guides; 2) expert consultation; 3) translation of topic guides; 4) risk assessment/mobilisation; 5) recruitment of participants; 6) piloting interviews; 7) modifying topic guides; and 8) reflecting on the process and reporting the pilot results (Figure 1).

Other authors have presented steps for interview guide refinement.18,24 However, to our knowledge, there is no methodological paper presenting operational considerations for conducting research in conflict settings across two or more countries with multiple languages in Africa. Some researchers have recommended good practices for piloting qualitative studies requiring translation in multiple languages in a bid to resolve discrepancies between translations and identify expressions that could be inadequate.25,26 However, these researchers are focused on aspects of the translation process that is valid in our research but does not address aspects of insecurity and other challenges that come with conducting research in humanitarian settings. The challenges are linked to obtaining security clearances from belligerents of conflict, recruiting participants for interviews, where poor communication networks, kidnapping and crossfires are on-going in these settings.
In this paper, we present the practical steps we took to validate our study’s feasibility and ensure the collection of good-quality data. The entire process from development to implementation was conducted from August 2021 to July 2022.
Step 1: Interview guide development
Three in-depth interview guides and one focus group discussion guide were developed with semi-structured open-ended questions. These four interview guides were developed to respond to specific research areas and different categories of respondents (Table 1). The first drafts of these interview guides were prepared in August 2021 following the systematic review. Questions in the interview guides were refined between May to June 2022. The interview guides were refined following the results of the cross-sectional study conducted as part of the larger research study. This enabled us to familiarise ourselves with the topics and existing gaps, as recommended by Morris.27
Step 2: Expert consultation
The draft interview guides were shared with three academic and two humanitarian experts in Cameroon and Nigeria to provide feedback on the wording of the questions, language and contextual relevance of the questions, and any cultural or other barriers that might arise. This is in line with recommendations from Majid and colleagues.20 More adjustments were made to the interview guides following feedback from experts. The feedback included suggestions such as simplifying technical words like “models of care” to “approaches/strategies”, adding diagrams to the fact sheet describing the different healthcare delivery approaches, collecting more demographic information about the participants, reformulating questions and/or probes, changing terms such as “community members” to “internally displaced persons/refugees”, and removal of probes that were duplicative. The expert consultations improved the initial refinement of questions for better clarity, as recommended by Majid and authors20 and Yeong and authors.18 Involving experts in reviewing the interview guides allows for different perspectives and insights into the probing questions to be included in the interview guides.
Step 3: Translation
Due to the cultural diversity of communities in Cameroon and Nigeria, several local languages are spoken. The decision had to be made on which language to use for interviewing, especially for displaced populations. For the Cameroonian context, because pidgin English (the local language) is commonly spoken by almost all residents in the North West and South West (NWSW) regions regardless of their tribe, pidgin English was chosen as the language of choice to be used for interviewing. Meanwhile, for the Nigerian context, Hausa, Kanuri and Fulfude are the local languages spoken by 31%, 38% and 11% of North East Nigeria (NEN) households, respectively.28 For the pilot, Hausa was chosen as the language in which interviews were to be conducted. Research assistants translated the interview guides. However, the back translation following piloting revealed that the translation in Hausa by the research assistants was poorly done, which impacted the quality of data collected during the pilot interviews. From the pilot phase, a decision was made to seek the services of professional translation of the final interview guides. The translation was only needed for interviews within these communities. All interviews with humanitarian organisations were done in the English language. Translation of the interview guides was very important to ensure consistency across both countries, though, during our piloting process, we did not engage professional translators when we piloted our interview guides. Mckown and co-authors25 recommend using professional linguists who have experience in translating as good practice for translating clinical outcome assessments.
Step 4: Risk assessment and community mobilisation
The World Health Organisation classifies the conflicts taking place in the North West and South West regions of Cameroon and North East Nigeria as grade two, protracted emergencies.29 Considering the insecurity of the contexts in which this research had to be piloted, a risk assessment had to be conducted on how best to collect quality data without putting the lives of researchers and research participants at risk. The risk assessments included how to mitigate risks from kidnapping, forceful retention and stray bullets. Also, assessments were made on the geographical, cultural, religious, communication, and logistical challenges recommended by Chaudhri and co-authors,30 for operations in conflict settings. Following the risk assessment, a decision was made to conduct all in-depth interviews with humanitarian organisations virtually. This modality was considered practical to meet the busy schedules of senior-level staff in humanitarian organisations whom the research largely targeted. For in-depth interviews and focus group discussions with internally displaced persons, face-to-face interviews in communities mapped as green or yellow in the risk assessment were considered a better option. Risk assessment was done using the risk template used by humanitarian organisations in Cameroon and Nigeria. Following risk assessment, online interviewing was considered the preferred modality as it presented the least risk. However, contextual reality linked with internally displaced persons (IDPs) not having easy access to laptops or the internet necessitated face-to-face interviews, especially for focus group discussions (FGD). Notwithstanding, the location of the FGDs was agreed upon with the communities to ensure they selected a location where they felt safe to meet in a group. This was facilitated by the access/security mapping and access mobilisation exercise conducted to identify locations where participants could safely converge for the interviews.
For in-depth interviews, the option of online interviewing in some cases was feasible but required that the IDPs be provided with a laptop and internet connection so that the interview could take from their place of residence.
Besides the risk assessment that was conducted, community mobilisation was done to gain access and acceptance of field activities by the State Armed Groups (SAG), and communities. This strategy was used to mitigate the risk of kidnapping or forceful retention of research assistants or participants. This consisted of providing information letters to SAGs and holding community meetings with community leaders to inform and discuss the research activities. The meetings held in communities were also meant to mitigate kidnapping by Non-State Armed Groups (NSAG) as information about the research would usually spread within communities. These community meetings were opportunity for the research participants to be informed about the research.31
Risks assessment and community mobilisation were done before the final two stages during the pilot process (Figure 1). That is, before the recruitment of participants and conducting field interviews with IDPs in the communities.
Step 5: Participant selection and recruitment
Recruitment of participants for the pilot phase was carried out using recommendations made by Reach Out Cameroon and Herwa Community Development Initiative which have had humanitarian operations in both countries. Study participants resided in Buea (South West Region of Cameroon) and Maiduguri (Borno state in North East Nigeria). Volunteers from humanitarian organisations were invited to participate in interviews by email. In contrast, study participants who were internally displaced were recruited with the help of community facilitators who assisted in the identification of internally displaced persons (IDPs) and host community members in Tole and Maiduguri. Participants in the pilot study shared similar characteristics as those to be recruited for the main study, as Persaud22 recommended.
Step 6: Interviewing
The interview guides were pilot tested with six participants purposefully chosen from humanitarian organisations and populations affected by the conflict in South West Region of Cameroon and North East Nigeria. Written and oral consent was obtained from all participants before the pilot interviews. Four of the interviewees were from humanitarian organisations, and two were IDPs. All in-depth interviews were conducted using Microsoft Teams, using both the recording and transcription functionalities on the platform. The duration of the interview ranged from 60 to 65 minutes. Two internally displaced persons selected for the interview via Microsoft Teams (Office 365 ProPlus), were connected to the laptops of the research assistants, enabling the participants to take part in the interviews from the comfort of their homes. For these IDPs, research assistants took laptops with internet keys to the participants’ homes and helped them log into the Teams meeting. Once the process of logging onto Teams was successful, the research assistants left participants in their chosen private space to continue with the call.
Handwritten notes were also taken in a diary by a second researcher while the interview was ongoing. All focus group discussions occurred face-to-face in the community where the internally displaced persons and host community members reside at a location chosen by the participants. Focus group discussions were piloted with a group of eight IDPs and host community members in Cameroon in pidgin English, while that of Nigeria was piloted in Hausa with a group of nine people. Focus group discussions lasted 60 minutes in each country.
All participants in the pilot received an internet voucher of £20 or transportation reimbursement of £20 as compensation for their time and effort in the study.
Step 7: Modifying protocols
Revisions were made to the topic guides by adding/removing some probing questions. Questions such as “Does the absence of a health facility influence which model of care (approach) is used to provide primary health care?” This question appeared twice in the topic guide under different sections. Another question which was repetitive and experienced as intrusive was "Which of these models of care (approaches) does your organisation typically use and why? Hence, probes that were repetitive and confusing were deleted. The fact sheet, which contained definitions of terms used during the interview, was simplified, and pictures were added to improve clarity in the version of question used for internally displaced persons or host community members.
Step 8: Reflecting on the process
Following the end of data collection for the pilot phase, a reflective process was engaged to draw lessons from errors made during the entire process with the goal of improvement. A key observation during the interview with participants from humanitarian organisations was that participants were protective of their organisations’ approaches to delivering health care. There was a need to take time to further explain to all participants in future interviews how confidential and anonymised the data collected would remain. Suggestions from Kaiser32 were applied during the interview process to build trust and rapport with study participants, but we may not have been efficient in applying the recommendations. We decided to take more time to discuss confidentiality issues with participants and improve rapport by presenting research updates in cluster meetings.
Limitations of the pilot
This pilot had a small sample size which may not have fully represented the diverse opinions and experiences of humanitarian organisations and IDPs. Notwistanding, interviews with a wide range of humanitarian organisations and IDP were planned in the bigger study.15 On two occasions the interview process was disrupted due to inadequate internet connectivity in Cameroon and Nigeria. Interviews resumed once participants could reconnect online.
DISCUSSION
Piloting research studies in conflict-affected settings is very important to ensure the safety of researchers and study participants. It also ensures the credibility and quality of the data collected.18 Previous authors have suggested interview guide refinement pathways,18,20,21 but these did not consider the specificities of conducting research in conflict-affected settings. We share an eight-step process to successfully refine interview topic guides for multi-country studies in conflict-affected settings involving several languages. Previous authors did not include two steps in our refinement process, which we believe are very important when conducting research in conflict-affected settings. These are: risk assessment, community mobilisation, and a reflective process. Conducting research in conflict-affected settings presents significant risks that can be mitigated by conducting a risk assessment of the communities in study locations and strongly engaging with the communities through mobilisations. This step is important not only because it is key in determining access to study participants, especially internally displaced persons, whose opinions and experiences are valuable in research conducted in these settings.
From this refinement process, key lessons were learned, and specific measures were taken to improve the interview process in the main study. These measures include: listening to the recorded tapes of the interviews, getting the protocols translated by professional translators, further simplifying words and terminologies, taking time to introduce the research and laying emphasis on the anonymity of the responses to encourage participants to provide open and frank responses and simplify the interview fact sheet for IDPs to include images of the models of care.
Piloting the interview process allowed for refinement of our interview guides, testing the questions to ensure participants could easily understand the questions, and improving the interviewers’ interview techniques. This process was helpful inin improving the reliability and validity of our interview guides.
Acknowledgements
We appreciate the staff from the humanitarian organisations and internally displaced people who took part in this pilot study. This research was made possible with the kind support of the Elrha Research for health in Humanitarian crises (R2HC) award. This work is also supported by the University of Cambridge Clare Hall Boak Student support fund, and the University of Cambridge Frere, Mosley and Worts Travelling Scholars Funds.
Ethics
Approval has been obtained from University of Buea Institutional Review Board, National Ethics Committee for Research in Human Health Cameroon, National Health Research Ethics Committee Nigeria and Cambridge Psychology Research Ethics Committee
Funding
This work is supported by ELRHA (grant no: CGA 70179), the University of Cambridge Clare Hall Boak Student support fund (NA), and the University of Cambridge Frere, Mosley and Worts Travelling Scholars Funds (NA). The funding sources had no role in the design and conduct of the study: collection, management, analysis and interpretation of the data; preparation, review and approval of the manuscript; and decision to submit the manuscript for publication.
Authors’ Contribution
LAO led the process of developing the interview protocol and the interviews and wrote the first draft of this manuscript. KO, TVB, NT, ZW, MNH, EO, AM, YP and RPR suggested edits to the interview protocol and manuscript. IM and GF conducted focus group discussions in communities. All authors approved the last draft.
Competing interests
The authors completed the ICMJE Disclosure of Interest Form (available upon request from the corresponding author) and disclose no relevant interests.
Correspondence to:
Lundi-Anne Omam, Department of Public Health and Primary Care, University of Cambridge, Cambridgeshire, United Kingdom. [email protected]