


One of the ways in which global health aims to distinguish itself from its predecessors, tropical medicine and international health, is an emphasis on equitable partnerships between “Northern” and “Southern” actors.1 Most global health programs are implemented in low- and middle-income countries; however, persisting power asymmetries between global health actors based in high-income countries (HICs) and those in LMICs have challenged the reality of equitable global health partnerships.2,3 These power asymmetries include the unequal distribution of resources, including finances, political authority and knowledge. Broader structural, political and economic inequalities have been cited as responsible for these asymmetries, ingrained in the legacies of colonial medicine and international health.4
In the international non-governmental organization (iNGO) space, power asymmetries often manifest through the exclusion of in-country actors in decision-making for health programs. This exclusion of in-country actors has been highlighted in various global health programs, including HIV/AIDS, Malaria, maternal health and non-communicable diseases.5,6 Excluding in-country actors and communities, intentionally or unintentionally, in the design of global health programs is problematic for several reasons. First, it can lead to a poor representation and understanding of the local realities and challenges being faced.7 Next, it can enforce a lack of ownership of developed programs for local actors and program users.3 Finally, sustaining interventions and programs conceived without the participation of in-country actors is often challenging due to the lack of ownership. Evidence suggests that projects designed in collaboration with communities to gain local ownership are generally more impactful and sustainable, especially after the original project funds are exhausted.8,9
Human-centered design (HCD) is a creative approach to problem-solving that includes the people one is designing for, and ends with solutions designed to address core needs by putting people at the center of the design.10 Design thinking is a HCD technique with an analytic, creative, and iterative problem-solving process that seeks to understand the end-users, challenge assumptions, redefine problems and create innovative solutions to prototype and test.11 The human-centered framework of design thinking allows for innovation and problem-solving by team members with diverse talents, skills, and knowledge. For all these reasons, HCD is increasingly popular in healthcare and global health as evidenced by the increased use in U.S. Agency for International Development (USAID) Development Experience Clearinghouse documents.10
The use of design thinking in global health has mainly focused on specific products and services, such as digital technology for mHealth. However, iNGOs could leverage its characteristics in the collaborative design of program design.12 This paper aims to recount efforts by Operation Smile, a surgical iNGO, to ensure equitable collaboration between in-country and international stakeholders during the co-creation of Operation Smile Malawi’s (OSM) five-year Strategic Plan. Specifically, it discusses how design thinking was used to ensure a collaborative environment and process in which in-country and international staff worked together to co-create the strategy. We start by summarizing the overall OSM strategic planning process, followed by how design thinking was used for decision-making. We finished with feedback from participants regarding their perception of the utility of design thinking and lessons learned.
Design thinking in Operation Smile strategic planning
Strategic planning context
Operation Smile Inc. (OSI) is a forty-year-old iNGO working to provide access to high quality surgical and comprehensive care to people with orofacial cleft lip and palate (CLP) conditions in over thirty LMICs.13 In general, the implementation of OSI programs occurs through locally registered NGO partners referred to as foundations, such as Operation Smile Malawi (OSM). These foundations are led and staffed by in-country teams and generally have independent in-country boards that oversee the implementation of programs. OSM is an OSI-affiliated NGO based in Lilongwe, Malawi.14
Operation Smile and its partners have provided care to over 326,000 people with CLP globally, primarily in LMICs through a short-term surgical mission model.15 In this care delivery model, medical volunteers, often from HICs, travel to LMICs to provide surgical care to patients at partner hospitals typically over a two-week period.16 Furthermore, Operation Smile’s care delivery model has evolved to include comprehensive care with significant investments towards strengthening health systems.17,18
In 2019, Operation Smile embarked on a global strategic planning process to define the vision and long-term goals for the entire global organization. To ensure that these goals were aligned with the local needs and priorities of its in-country partners, OSI advised each foundation to define gaps in CLP and surgical care delivery and identify contextual long-term solutions for these challenges in alignment for the vision of the organization.
METHODS
Strategic planning process
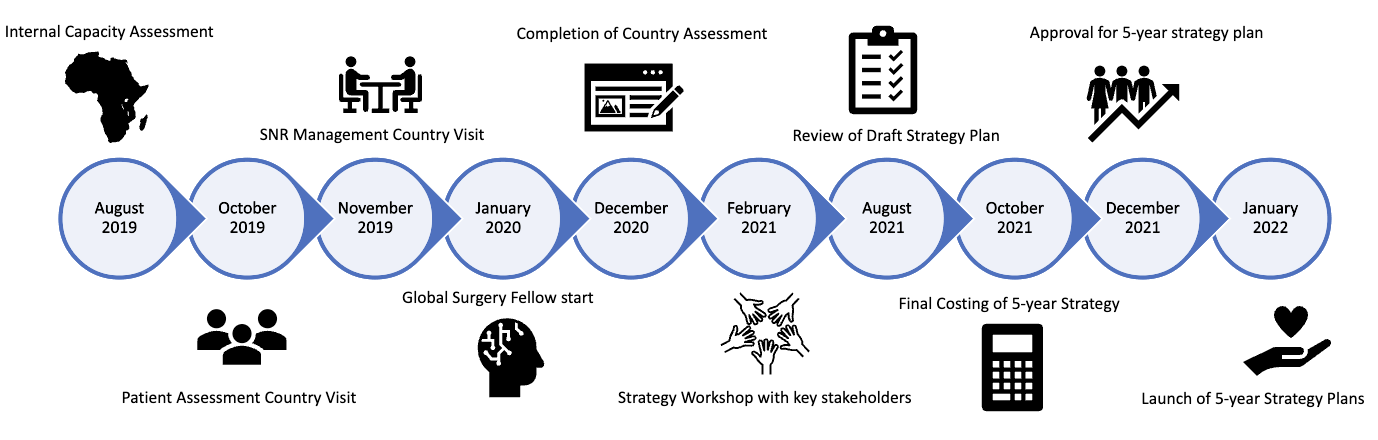
OSM embarked on its strategic planning process in August 2019. The initiative was co-led by OSM’s country manager and an adviser from OSI (DM and DTJ). It began with the analysis of strengths and gaps of the CLP care capabilities and the surgical system in Malawi (figure 1). This was followed by an inclusive priority setting workshop using a design thinking framework to determine the goals, priorities and activities of OSM’s five-year strategic plan.

Situation analysis
OSM’s situation analysis aimed to gather information relevant to CLP and surgical care in Malawi and advance an evidence-based and data-driven strategic plan. Data sources included peer-reviewed literature, grey literature, public health leader interviews, and field visits to partner hospitals and all four tertiary hospitals in the country. Data from hospital visits was collected using the modified World Federation of Societies of Anesthesiologists hospital assessment tool.19
Priority setting workshop
After the situation analysis, OSM staff and partners were invited to a hybrid virtual/in-person workshop to deliberate on the priorities of OSM’s five-year strategy. The workshop was held over a four-day period from 15th - 18th February 2021 in Lilongwe, Malawi. The Microsoft Teams platform was used by participants attending virtually (Figure 1).
This priority setting workshop was led by the OSM leadership and moderated by four individuals: two at the physical location (CM and DM) and two remotely (DTJ and USK). The moderators used an adapted design thinking process to ensure a collaborative approach to decision-making around the goals and strategies for OSM’s five-year strategic plan. In-country participants included 11 local staff members working in finance, administration, partnership and fundraising, volunteer recruitment and patient coordination and 2 clinicians from Malawi. All 11 local staff members make up the entire staff for Operation Smile Malawi, the workshop aimed to have 100 percent of staff members to participate in the strategic planning and proactively decide what the would focus on for the next five years based on their areas of expertise and work. Five international stakeholders participated, namely one global surgery fellow, one fundraising partner, a regional director, one regional coordinator and one health policy consultant that support and work with the Malawi team.
We chose a design thinking framework consisting of four iterative questions to steer the process: "What is", “What if”, “What wows”, and “What works” (Figure 2).20,21 This framework was chosen among numerous design thinking frameworks, because it lent itself to collaborative answering of key questions needed to develop the OSM long-term strategy. The framework flows logically from openly exploring the current situation (what is), to imagining possible innovative solutions (what if), to prioritizing solutions (what wows), and defining actionable interventions (what works).

During the process design tools that were used included visualization, journey mapping, mind mapping, brainstorming and concept development. Throughout the strategic planning workshop, LucidChart software and Microsoft Teams were used to visualize each process.21
In this four-step process, the first step, "What is" aims to assess the current reality. During the workshop, the OSM team reflected and shared their experiences of the current CLP and surgical landscape in Malawi. The process was supplemented with findings from the situation analysis. Moderators led one and a half day of discussions and mapping of the current state of CLP and surgical care in Malawi from the perspective of the participants (see figure 3 for a sample mind map).

The discussions included an evaluation of the available infrastructure, health workforce challenges and support related programs, the capacity of partner hospitals and patient barriers. Fundraising efforts and partnerships were also discussed.
The subsequent “What if” step used findings from the "what is" process and encouraged participants to envision multiple options for creating a new future without hindrances such as limited resources. Participants were separated into five small groups and asked to create at least two "what if" statements about what they would like to see OSM accomplish based on the reality of the current situation that was mapped out in the "what is" step. These statements were then reported back to the larger group and aggregated into categories. Examples of "what if" statements included; what if OSM could do surgery through surgical programs with fully formed local teams?; what if OSM could invest in cleft and surgical education in Malawi in order to increase local capacity? Other examples are presented in figure 4.

Next, the “What wows” step prompted the team to prioritize "what if’’ statements. Concept development and mind-mapping was used at this stage to concretely identify key areas of focus for OSM’s strategy. Five core "what if’’ statements were identified as priorities for the strategic plan by participant consensus; 1) what if OSM made comprehensive cleft care available to everyone in need in Malawi; 2) what if OSM invested in cleft and surgical education in Malawi in order to increase local capacity; 3) what if OSM invested in infrastructure, equipment and supplies to strengthen local capacity; 4) What if OSM strengthened local information management systems and, research and innovation for better patient care and impact assessment and; 5) what if OSM contributed to cleft and surgical policy and advocacy in order to scale impact. By envisioning the possibilities following the "what if’’ process, the “what wows” prompted the team to think about which solutions are practical. For example, what infrastructure investments will create the most impact in the way surgical services are delivered? How can the team collect information that promotes evidenced decision making and aid monitoring processes?
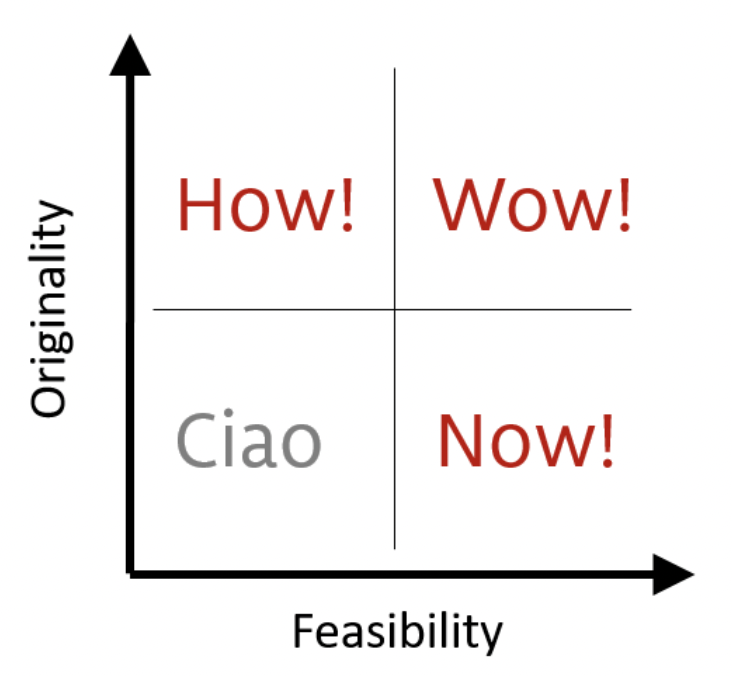
Finally, in the "what works" step, we focused on concretizing the five “what if” statements into actionable activities that would be implemented over a five-year period. Mind-mapping was again used along with brainstorming as design tools. Activities that were included in the final strategic plan were narrowed down using the How-Wow-Now Matrix (figure 5). This matrix helped assess proposed activities in accordance to the team’s perceived feasibility and originality as the main category for prioritization. After each suggested activity was passed through this matrix, those with high originality and feasibility (wow!) were deemed innovative and ready for implementation (within 1 to 2 years). Those with high feasibility and low originality (now!) were considered low risk and with potentially high acceptability to be implemented within 3 years. High originality and low feasibility activities (how!) were considered for later implementation (3 to 5 years), while low feasibility and low originality ideas (ciao!) were eliminated from the strategy as agreed by team members. The final list was organized into objectives, strategies, and outputs, along with an activity matrix by a smaller group after the workshop.

RESULTS
Participant feedback
After the workshop, the moderators collected the team’s feedback on the design thinking strategic planning process via an e-survey. The 27-question e-survey assessed the participants’ understanding and perception of the design thinking process (Supplemental File 1). Eight out of eleven the in-country stakeholders who participated in the strategic planning workshop completed the survey. Sixty percent (n=5) of respondents had never participated in the development of a strategic plan at OSM before and half of the participants (n=4) had never heard of design thinking before the workshop. Most participants (62.5%, n=5) responded that the concepts/process of design thinking was clearly explained to them and the rest reported that that process was only partially explained (37.5%, n=3). All respondents also reported that the workshop objectives were clearly explained by the facilitators. Two respondents (25%) felt their experience was “excellent” and the rest rated it as being “good experience” (n=6). Three participants (38%) stated that their expectations were fulfilled while the rest stated that their expectations were only partially fulfilled (62%, n=5). Almost all (n=7) respondents strongly agreed that the facilitators sustained the group’s interest and participation, and 62% (n=5) strongly agreed that the facilitators answered all the participants’ questions.
Most (87%) respondents rated their team’s engagement as “above average” during the workshop and one participant rated the engagement as “excellent”. Most respondents (75%, n=6) rated their own level of participation during the workshop as either “excellent” or “above average” while the rest rated their level of participation as “average”. Three quarters of the respondents (n=6) stated that the workshop had an effect on their understanding of teamwork and all participants either rated the level of team spirit during the sessions as excellent or above average.
At least three quarters of participants stated that all parts of the chosen design thinking framework were effective. All participants agreed that the design thinking process made the strategic planning workshop productive. All participants also agreed that the design thinking process helped them incorporate their own ideas into the five-year strategy. Similarly, all participants responded that the strategy workshop helped them to better understand OSM’s long-term strategy. Furthermore, all participants reported they had learned something new outside their area of expertise.
When asked, in an open-ended format, what they liked the least about the design thinking workshop, some participants felt that there was not enough time for the workshop while others believed that the workshop was too prolonged and tedious. Other participants stated that the hybrid nature of the workshop made the communication with virtual participants more tedious. These participants believed having everyone attend in-person would have been better and more productive; however, they felt that overall, the workshop was still effective. One participant felt there were not enough volunteers, patients, and donors at the workshop. Several participants stated that the workshop would have been more productive had the facilitators broken the team into smaller workgroups at the start of the session as the larger group discussions were less productive.
The survey was an optional activity for participants, and it took on a qualitative approach. It is therefore difficult to determine if non-response affects the findings. Moderators reached out all participants more than once to make sure that participants were able to give their feedback should they want to and assured them that their responses were anonymous. It was however communicated before and during the workshop that we choose this method of strategy design for inclusivity and that all thoughts and opinions mattered to the effect of developing a human-centered designed strategy and true collaboration.
DISCUSSION
While Human-centered design (HCD) and specifically, design thinking has been used and extensively described in the business sector and other fields, its application in global surgery has scantly been documented. This paper recounts the initial use of design thinking to foster open collaboration during the co-creation of a long-term strategic plan for OSM. It also details the effect of the design thinking process on the participants’ engagement in the decision making process and taking on their suggestions for improvement. Together, this information enriches the discussion around the practical applications of HCD and design thinking in global health.
The application of HCD in global health is increasingly popular.22 Its increasing popularity has led to the creation of the Design for Health initiative by USAID and the Bill & Melinda Gates Foundation.23,24 To the best our knowledge, this paper is the first to report HCD in global surgery, specifically focused on the use of design thinking for strategic planning. Furthermore, this paper focuses on the experience of Operation Smile, an iNGO, which could be applicable to other iNGOs and institutions in global surgery and global health.
In their commentary, Andrawes, Johnson and Coleman argue that HCD in global health can foster interdisciplinarity in three ways: “1) integrating explicit and implicit knowledge; 2) challenging linearity with iteration and; 3) enabling collective ownership of processes and solutions.”25 The types and uses of knowledge in global health including who wields expertise has frequently been challenged.25–27 When the lived experiences of in-country partners, end-users and communities are excluded in the development of global health interventions and programs in favor of foreign ‘expertise’, poor, incomplete or inaccurate understanding of local problems and eventually can lead to ineffective and unsustainable programs. In the OSM strategic planning process, design thinking enabled the incorporation of knowledge/evidence from scientific/global health inquiry through the situation analysis and the experiential knowledge of in-country staff and partners. Specifically, the “what is” section which used mind mapping allowed stakeholders to map out challenges and solutions to CLP and cleft care in Malawi. Feedback from the stakeholders shows agreement that the design thinking process enabled them to incorporate their own ideas into the strategic plan. It hints that the process enabled implicit knowledge to blend with the perspectives/tacit knowledge of the in-country staff and partners.25
Design thinking is built on a profound interest in developing an empathetic understanding of the people for whom the products or services are designed.11 It fosters teamwork, open-mindedness, and finding solutions by leveraging the participants’ experiences and expertise with an emphasis on the end-user.22 Collaboration is integral to the design thinking process - it brings together individuals, communities and organizations to co-create and implement solutions.25 This approach allows multiple voices to be heard and incorporated into the development of solutions.
During the OSM strategic planning process, collaboration was fostered by creating a safe environment for active participation from all participants. The in-country team oversaw the process of organizing, setting the agenda, and determining priorities for the OSM strategic plan. The moderators promoted a flat organization structure of interaction during the workshop, which means that hierarchical relationships were of no effect and by intentionally grouping participants to random teams, they would have diverse perspectives and encouraged initial critique of proposals during the ideation phase.
In-country actors provide the required context and important organic lessons from previous and similar endeavors that foreign actors often lack. In this paper, the in-country actors contributed significantly to the situation assessment and the participants were encouraged to set aside limitations when they proposed goals during the “what if” phase. These conditions facilitated the identification of novel insights and solutions. As a result, we noted a trend from the traditionally service delivery-oriented plans to a more comprehensive health system strengthening approach. Similarly, Bruns et al., found that the integration of HCD in the design of an HIV program targeting men in South Africa was helpful in identifying the most valuable components in their program according to end-users.28 Design thinking challenges assumptions international actors have before they commit to investments and ensures end-users are a part of every process.
From a theoretical standpoint, this paper had all the key elements of a HCD in global health and theory of change.29 We set out to improve access to safe, timely, and affordable surgical care for Malawian patients and to build a strategic plan by and for Malawians (global health ecosystem goal). As a result, we developed an adaptive, sustainable, and contextually appropriate plan. In addition, this exercise increased HCD expertise and experience among participants as evidenced by the survey results.
The OSM team co-led the entire process with partners from OSI and all aspects of the situation analysis were designed and led by members of the OSM team. The early identification and inclusion of stakeholders, as well as a flat organization approach in conduct created a safe space, and empathy was also a vital ingredients to the HCD process.29 As such, it is recommended HCD should be organized before project development and grant applications to ensure that solutions developed address the users’ actual needs and that the users’ are actively involved in the project thereby promoting buy-in. In their lessons on the application of HCD in global health, Blynn et al., advised that establishing ownership at the beginning of a project was valuable for buy-in and sustainability.30 We observed this to be true in our project.
The ongoing COVID-19 pandemic has challenged how we practice and collaborate on global health. With restrictions on travel, international partners were not able to travel to Malawi for the OSM strategic planning workshop. However, using available digital visualization technologies like LucidChart and Microsoft Teams, equitable collaboration using design thinking was still possible. While feedback suggested that some OSM members would have preferred an all in-person workshop, they still indicated that the hybrid model was effective. Therefore, our project showed that it is possible for international and local partners to collaborate in meaningful ways virtually.
Since design thinking is an iterative process, it can be time consuming. Some participants noted that more time was needed for the entire workshop. Therefore, future designers should be flexible to allot enough time to the design process. Alternatively, the participants suggested that splitting the group up into teams during certain parts of the process, such as brainstorming "what if" statements, could allow for more efficient use of time.
Limitations
The design thinking workshop consisted of 17 individuals with different roles in the organization, 4 of the individuals were leading the process and 9 were local staff that were from different departments. Because they are few in numbers, most of the departments have one person each, although the patient coordination team is made up of 4 team members, 3 of which are split across the three regions in Malawi and 1 who is the national coordinator. The sample number of the experience of the design thinking workshop therefore inadequate to make a definitive stance on the use of design thinking.
In the future, the process could benefit from the participation of community volunteers, especially patients and patient advocates. Since the process of design thinking thrives on its human centered approach, it also requires a thorough and timely process. Of note, the literature on the use of design thinking in health is scarce since it has traditionally been used in other industries with much success. We hope that this paper contributes to the availability of literature in this area.
CONCLUSIONS
Human-centered design is vital for framing problems and developing solutions that are centered on people in their context. More than 400 NGOs provide surgery, obstetrics, anesthesia and trauma care in LMICs.31 The majority of these organizations are headquartered in HICs and have senior leadership from HICs.31 As such, their understanding of the local needs and priorities may be clouded by assumptions and biases. Just as has been shown here, HCD and design thinking can be used by iNGOs to foster collaborative creation of programs between local and international actors, such that these programs are based in a deep understanding of local context and the critical promotion of local ownership.
Acknowledgements
We are thankful for the time and dedication from the Operation Smile Malawi staff who worked tirelessly to develop the long-term strategy and provided feedback on the entire planning process. This includes; Joey Mdumuka, Elizabeth khuzakhuza, Melissa Mungomo, Idah Sitima, Fyness Zakeyu, Maurice Gomani, Harlod Nkhoma, Margaret Chigwenembwe, We also acknowledge the support of OSI leadership and staff including Karen Jacques, Sabrina Ghiddi, Tamlin Abrahams, and Bill Magee, and William P Magee for their contributions during the entire planning process. We acknowledge Caroline Yao and Allyn Auslander who reviewed the manuscript and provided feedback.
Funding
The OSM strategic planning process was funded by Operation Smile.
Authors’ contributions
DTJ is the study guarantor; CM, DTJ, USK conceptualized the study, designed study tools and analyzed the data and drafted the first manuscript. All authors reviewed, provided critical feedback and approved the final manuscript.
Disclosure of interest
The authors completed the Unified Competing Interest form at http://www.icmje.org/disclosure-of-interest/ (available upon request from the corresponding author), and declare no conflicts of interest.