At the time when COVID-19 was declared a pandemic in March 2020, its spread in the African continent was slow.1 However, confirmed cases of the virus have since risen steadily over the years in the African continent.1 The rapid spread of SARS-CoV-2 was due to numerous characteristics, including high transmission rate, asymptomatic persons’ ability to shed the virus to the environment, many persons with mild symptoms transmitting the virus, emerging new variants, and super-spreading events in many communities in Africa.2,3
Poor public health practices, disbeliefs, myths, negative perceptions, vaccine hesitancy, misconceptions about the virus, its origin, imported cases, and high COVID-19 vaccine hesitancy in many African communities were the other reasons for the rapid spread.2,3
There is a need for more information on COVID-19 vaccine acceptance in Ugandan population because there is misinformation and disinformation on the vaccine circulating in Ugandan social and mainstream media.4 For example, the most trusted source of coronavirus information among age-groups in Ugandan population differed, whereby younger age-groups rely on radios and other sources.5 In contrast, older people rely on coronavirus information mainly from the Government of Uganda, internet, social and mainstream media.5 This scenario creates differences in knowledge and perceptions on COVID-19 vaccines and acceptance among different age-group populations considering the many conspiracy theories, misconceptions, myths, negative perceptions, and disbeliefs in many African communities.6
According to the World Health Organization (WHO), vaccine acceptance is the degree to which individuals accept, question, or refuse vaccination.7 It determines the uptake rate and vaccine distribution successes in a community.7 So, as mass inoculation program of COVID-19 vaccines began in the African continent, one potential impediment was vaccine hesitancy (i.e., the unwillingness to receive COVID-19 vaccines).8,9
Recently, issues on vaccine hesitancy were heightened when a systematic review on vaccine hesitancy suggested that the willingness to accept COVID-19 vaccines ranged between 27.7 to 91.3% from Congo to China, respectively.10 Factors such as age, educational status, gender, income, residency, occupation, marital status, race/ethnicity, perceived risks of COVID-19, trust in healthcare system, health insurance, norms, attitude towards the vaccine, perceived benefit of vaccines, perceived vaccine barriers, self-efficacy, up-to-date on vaccinations, having tested for COVID-19 in the past, perceived efficacy of the COVID-19 vaccine, recommendation for COVID-19 vaccination, political leaning, perceived severity of COVID-19, perceived effectiveness of COVID-19 vaccine, belief that vaccination makes them feel less worried about COVID-19, believing in mandatory COVID-19 vaccination, perceived potential vaccines’ harm, presence of chronic disease, confidence, COVID-19 vaccine safety concerns, working in healthcare field, believing vaccines can stop the pandemic, fear about COVID-19, cues to action, COVID-19 vaccine hesitancy, complacency, and receiving any vaccine in the past 5 years were associated with the willingness to receive COVID-19 vaccines.10–12
So, differences in perceptions on COVID-19 vaccines among age-group populations create challenges for health managers on vaccine distribution and uptake in communities in northern Uganda. This study aimed to determine factors associated with perceptions on COVID-19 vaccines among different adult age-group populations in northern Uganda.
METHODS
Study design
We conducted a cross-sectional study in northern Uganda from March to April 2022. This study was part of a bigger study to determine factors associated with vaccine hesitancy/acceptance among adult populations in northern Uganda.
Study sites
This study took place in twenty-four health facilities in nine districts of the Acholi sub-region in northern Uganda; Namukora HC IV, Kitgum Government, and St. Joseph’s Hospitals in Kitgum district; Padibe HC IV, Palabek HC III, and Madi Open HC IV in Lamwo district; Pajule HC IV, Lacekocot HC IV and Pader HC III in Pader district, Kalongo Hospital and Patongo HC IV in Agago district; Lalogi HC IV, Opit HC III and Odek HC III in Omoro district; Anaka Hospital and Koch Goma HC III in Nwoya district; Atiak HC IV, Pabbo HC III and Amuru HC III in Amuru district, St. Mary’s Hospital Lacor, Independent Hospital, Gulu Regional Referral Hospital in Gulu City; Awach HC IV and Cwero HC III in Gulu district. These health centers were selected because they were involved in COVID-19 vaccination to the region’s population.
Study population
We recruited participants (adults/>18 years old) who were clients or attendants of outpatient clinics of twenty-four selected health facilities in the Acholi sub-region for illnesses other than COVID-19.
Selection criteria
The selection of participants was stratified at the regional level into the nine districts of the Acholi subregion and at the district level into twenty-four health facilities (Hospitals, HCIVs, and HCIIIs). In each health facility, the study was conducted in the outpatient department (OPD), where participants were selected by systematic sampling method in which every third adult attendee or attendant aged 18 years and above who consented to the study was recruited. Participants who were critically ill and could not answer research questions were excluded.
Sample size estimation
The sample size was calculated using Raosoft sample size calculator. The computation is based on a 50% response distribution, 5% margin of error, and 95% Confidence Interval (CI). This online software formula is for descriptive study sample size estimation.13,14 The research team chose this software calculator because Raosoft, Inc. form and survey software comprise a database management system with great strength and reliability that communicates with other proprietary formats. In addition, Raosoft database is a highly robust, proven system with high data integrity and security.13,14
The sample size was calculated using the formula
Based on the assumption of a population size of 45,000 clients and attendants in one month in OPD in twenty-four health facilities in the Acholi subregion, the minimum sample size based on the above assumptions was 396 participants.
Sampling technique
We used stratified sampling approach at regional, and district levels and systematic sampling approach for selecting participants at each health facility outpatients’ departments.15 The Acholi subregion was stratified into nine districts (Gulu City, Gulu, Nwoya, Amuru, Omoro, Pader, Agago, Kitgum and Lamwo districts) and into twenty-four selected health facilities (Hospitals, HCIVs and HCIIIs) where COVID-19 vaccines were being administered. At each of the twenty-four health facility outpatients’ departments, every third attendee or attendant was selected systematically for a period of one week until the required sample size was achieved.15,16
In the selected health facilities’ outpatient departments, it was estimated that approximately 45,000 people receive health services in one month. In this, we defined a systematic sampling as a probability sampling method where researchers select members of the population at a regular interval.15,16 We chose this sampling technique because it allowed us to get the desired sample size in the shortest period thereby reducing the risk of our study team acquiring COVID-19.
In addition, we chose health facilities because it was the most convenient place to receive participants as most population were still apprehensive to receive visitors/researchers in their homes, offices or public places as the lockdown measures had just been eased by the Government of Uganda and the population were still in fear of contracting the virus. Also, outpatients’ departments of health facilities had the required facilities for IPCs and SOPs that allowed interviewees and interviewers to interact while following COVID-19 standard protocols. Lastly but most importantly, systematic sampling method helps to minimize biased samples and poor survey results in addition to eliminating clustered selection with a low probability of obtaining contaminating data15,16 which was the ideal situation the research team had to achieve.
Study variables
Variables in this study were participants’ perceptions on COVID-19 vaccines and vaccinations. There were seventeen perception questions and statements on COVID-19 vaccines, which were designed on a five-point-Likert scale categorized as strongly agree “SA”, agree “A”, neutral “N”, disagree “DA”, and strongly disagree “SD”. See Box 1 for the seventeen questions and statements.
Data collection
Our research team collected data from participants using face-to-face questionnaire interviews, strictly following Uganda’s standard COVID-19 infection, prevention, and control (IPC) guidelines. We used a questionnaire constructed in English and consisted of questions on participants’ perceptions on COVID-19 vaccines and vaccinations in the Acholi sub-region (Additional file 1). The study instrument (questionnaire) was developed, grounded on literature reviews and discussions with the research team.17,18 Study participants were recruited by a systematic sampling approach at twenty-four health facility outpatients’ departments by our research teams. Every third attendant or attendee of OPDs were selected for interviews every day for a week until the required sample was obtained. Before data collection, the questionnaire was pretested among outpatients in Gulu Regional Referral Hospital, a hospital situated in northern Uganda. The internal validity of the questionnaire was determined as Cronbach’s α= 0.772. Furthermore, the questionnaire was designed to minimize lethargy in participants’ responses. In addition, participants were assured of confidentiality and privacy of their responses to reduce potential biases introduced by self-reported data and the fear of reprisals.
Data management
Data obtained from participants were de-identified. Only the principal investigator and supervisors had access to and were stored in a database with restricted access. The database was later archived at the Department of Surgery, Faculty of Medicine, Gulu University.
Data analysis
We analyzed this data using SPSS statistical software version 25.0. Age-groups of participants were presented in means, standard deviations, variance, standard errors, kurtosis, skewness, medians, ranges, and interquartile ranges. Data on participants’ perceptions on COVID-19 vaccines were presented as frequencies and percentages.
Responses on perceptions to COVID-19 vaccines were coded as binary dependent variables: “in agreement” for responses “Strongly agree and Agree” and “not in agreement” for “Neutral, Disagree and Strongly disagree.” The reference category for the dependent variable was “not in agreement.” A binary logistic regression analysis was performed with the age category (age-group less than 20 years as the reference category) as the independent variable against each perception variable as the dependent variable. Odds ratios with their corresponding confidence intervals were reported together with p values at a 95% significance level.
Ethics approval
This study was approved by St. Mary’s Hospital Lacor IREC (LHIREC No. 0192/10/2021). We obtained informed consent from each adult study participant. The research team-maintained confidentiality of participants’ information, and all residual data of participants were de-identified, kept under lock and key, and archived in the Department of Surgery, Faculty of Medicine, Gulu University.
RESULTS
This study achieved a questionnaire response rate of 723/396 (182.6%). Overall, 723 adult populations in northern Uganda participated in this study with a mean age of 31.4 years (standard deviation, SD, +10.1). The majority 54.5% (n=394) were males. The characteristics and numbers of participants in each age-group population were presented. In the less than 20 years, 41(5.67%); 20-29 years 318(43.98%); 30-39 years 225(31.12%); 40-49 years 95(13.14%) and >50 years 44(6.09%) (Table 1).
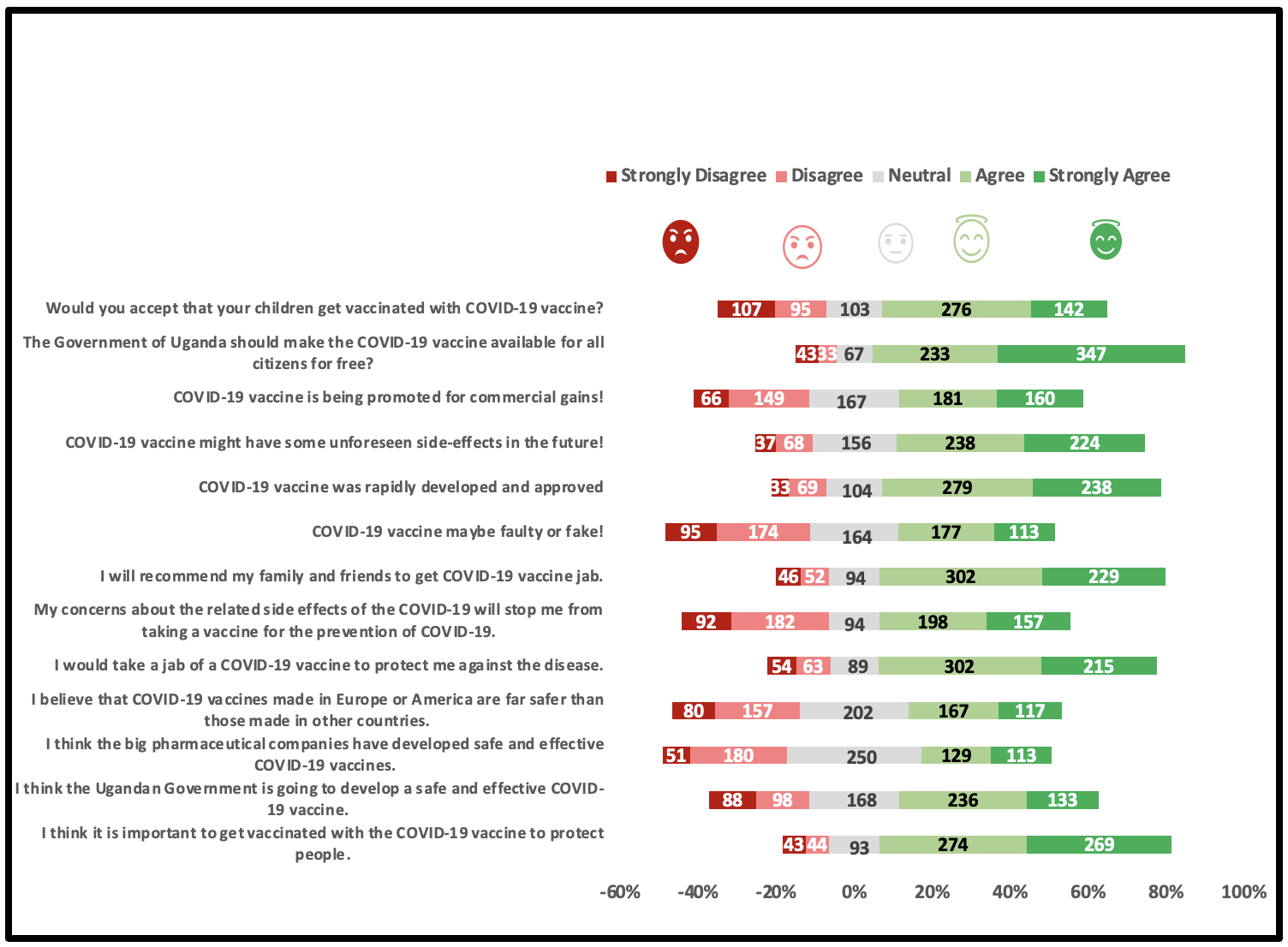
In addition, perceptions of the study population on COVID-19 vaccines were examined, and most participants’ responses were “strongly agree” or “agree” (“in agreement”) (Table 2).
Figure 1 is a Likert scale analysis of participants’ perceptions on COVID-19 vaccines (expressed in whole numbers). It shows that most participants either strongly agreed or agreed with questions and statements on COVID-19 vaccines and vaccinations.

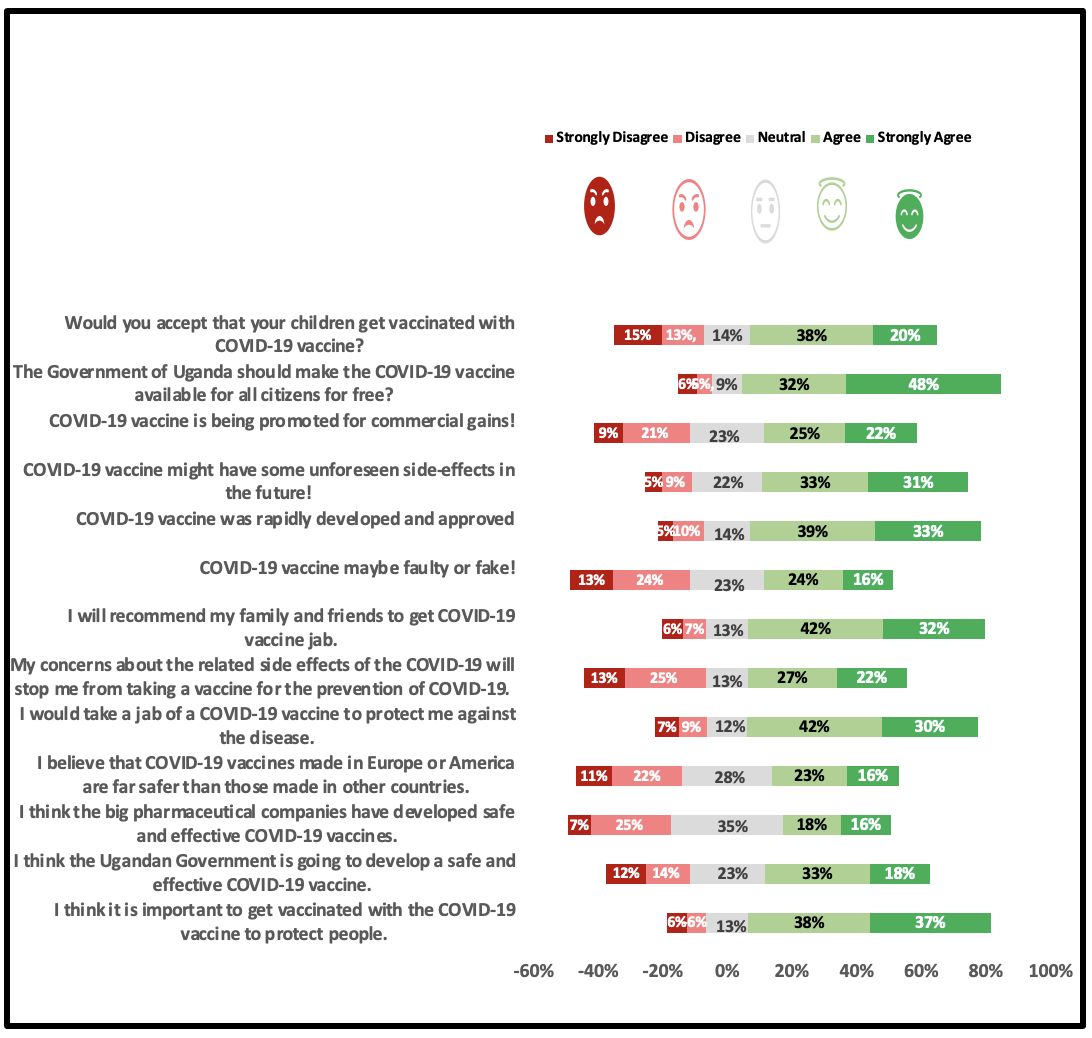
Figure 2 is a Likert scale analysis of participants’ perceptions on COVID-19 vaccines (expressed as percentage responses). It shows that a high percentage of participants agreed and shared similar perceptions on COVID-19 vaccines.

A multivariable logistic regression analysis of participants’ perceptions on COVID-19 vaccines are presented here where most participants agreed that it was important to take COVID-19 vaccines to protect themselves (adjusted odds ratio, aOR=1.02, 95% confidence interval, CI=1.00-1.04) compared to participants who did not agree. COVID-19 vaccines have an unlikely unforeseen side effect (aOR=0.98, 95% CI=0.97-0.99) compared to those did not agree; COVID-19 vaccines were unlikely to be promoted for commercial gains (aOR=0.98, 95% CI=0.97-0.99) compared to participants who did not agree; participants would accept their children taking a COVID-19 vaccine (aOR=1.02, 95% CI=1.00-1.03) compared to those who did not agree. Using less than 20-year-olds as the reference category and participants stratified by age-group populations, the 20–29-year-old perceived that COVID-19 vaccines developed in Uganda were unlikely safe and effective (aOR=0.59, 95% CI=0.35-0.97) compared to those who did not agree; COVID-19 vaccines have likely unforeseen side effects (aOR=2.14, 95% CI=1.29-3.57) compared to those who did not agree; and the >50 year old perceived that COVID-19 vaccine was unlikely being promoted for commercial gains (aOR=0.22, 95% CI=0.09-0.55) compared to those who did not agree.
DISCUSSION
The most significant finding from this study is that perceptions on COVID-19 vaccines among participants stratified by age-group populations are not substantially different (Table 1, Table 2, Table 3). Although two previous studies on perceptions of COVID-19 vaccines showed that different age-groups received COVID-19 vaccines and vaccination information from different preferred sources, older age-groups were more willing to accept COVID-19 vaccines than younger ones5; however, in our study, there was no significant difference (Table 3). The 2021 study in Ohio, USA, found that younger age-groups were less likely to accept the COVID-19 vaccine.19 The Ohio findings contrast with one in southwestern Uganda, which found that younger age-groups were more likely to take COVID-19 vaccines.20 These inconsistent findings in the two studies about the association between age-group categories and COVID-19 vaccine acceptance raises the need for more research on the influence of contextual issues such as differences in countries’ socio-economic dynamics, population structures, cultures, beliefs, perceptions, and understanding of COVID-19 vaccines in different geographical regions and peoples.
Nevertheless, the uniform and lack of perception differences on COVID-19 vaccines among age-group populations in our study is essential as the community can be engaged and sensitized to accept COVID-19 vaccines using the same method of information delivery in future COVID-19 vaccine rollouts. In addition, it will not require the Ugandan Ministry of Health to make special arrangements for vaccination campaigns for any age-group as all agree on the importance of COVID-19 vaccines and vaccination (Figure 1, Figure 2, Tables 1, Table 2, and Table 3). This current finding is not different from other studies, for example, in Uganda21 and Ontario, Canada,22 and among medical students in Sudan.23
There were several determinants of perceptions on COVID-19 vaccines among our study population (Table 3). Of particular interest was that they agreed that COVID-19 vaccines protect them against coronavirus, a finding like other Ugandan studies4,20,21 and African countries.10,23 Previous studies show that where a population had a high-risk perception of COVID-19, they readily accepted COVID-19 vaccines and vice versa.10,11 The intensity of COVID-19 second wave in Uganda, the personal understanding and experience of the illness, and the high mortality rates among high-profile personalities witnessed by communities in northern Uganda may have aided communities’ good perceptions on COVID-19 vaccines (Figure 1, Figure 2).
Secondly, the fear of unforeseen vaccines’ side effects was another factor that determined the community’s perceptions on vaccines developed against coronavirus (Table 3). The numerous side effects, including the fear of death, blood clots, mental health complications, and general body weakness have been extensively reported in other studies.10–12 Although many participants expressed concerns about the unlikeliness of vaccines’ side effects, there were substantial perception differences among participants stratified by age-group populations (Table 3). Participants’ responses were that the related side effects of COVID-19 vaccines would not stop them from taking COVID-19 vaccines or prevent their children from taking COVID-19 vaccines (Table 3). These findings do not agree with many studies in Uganda and elsewhere, where the fear of possible side effects of COVID-19 vaccines led to vaccine hesitancy.20–22
We, the authors argue that the mass education, sensitization, mobilization, and community engagement that the Ugandan Ministry of Health conducted before our study allayed these fears of vaccine side effects. Mass mobilization of communities on COVID-19 vaccine acceptance must be undertaken for successful COVID-19 vaccine campaigns in the future. In addition, we, the authors propose that prompt and timely provision of remedies to vaccine complications at the nearest health facility by village health teams will minimize vaccine side effects and uptake concerns.
The willingness of community members to privately pay for COVID-19 vaccines was not substantially different among age-group populations and has raised great interests (Table 3). Most participants in this study population and like another in northern Uganda had no health insurance coverage except a few educated white-collar workers.4 This finding has raised the interest of the authors that most study participants were not covered under any health insurance scheme.4
In epidemics/pandemics, people find themselves at crossroads regarding how to deal with costs of treatment for infected persons. We, the authors argue that the lack of health insurance coverage among most Ugandans is a time- bomb ready to detonate soon. The country is experiencing increasing incidence and prevalence of infectious diseases, non-communicable ailments, and lifestyle diseases. The Ugandan Government could avert this situation by legislating on the proposed Health Insurance Scheme Bill, which the Ugandan Parliament passed a year ago but has yet to be enacted into law. The astronomical medical bills served to clients in private health facilities during the treatment of COVID-19 patients were some of the challenges noticed during the second wave of COVID-19 in Uganda. A single person’s treatment for two or more weeks ranged between $20,000-40,000, which was unaffordable for many Ugandan patients. The lack of health insurance coverage other than the out-of-pocket payments was a serious challenge, depleting hard-earned resources and leading some families to acute debts and ultimately down the poverty line. We, the authors argue that the sooner this country discusses the national health insurance bill and enacts it into law, the more likely the population will suffer from more severe resource depletion in treating diseases such as COVID-19.
Remarkably, children taking COVID-19 vaccines was a determinant factor among participants (Table 3). The general opinion among community members was that vaccination of children against the virus should go ahead (Table 3). However, previous studies in the same setting noted that the coronavirus did not cause severe disease in children and young adolescents below 20 years.4,24 This finding aligns with many studies in Uganda, where children experienced milder forms of the disease with limited symptoms, symptoms’ burden, and duration of illness.24,25 These findings among Ugandan children are encouraging information that the Ugandan Ministry of Health could use to inspire children to adopt other public health approaches, such as wearing facemasks instead of mass COVID-19 vaccine rollout among these age-group populations.24
However, with many uncertainties about the virus and the possibility of emergence of new variants in an unvaccinated population, some scholars and physicians argue that it would be unwise for a country to rely on the current findings on children. This argument is because new variants may emerge and affect the unvaccinated population, thus, destroying the successes already achieved by the Ugandan Ministry of Health. Because of many uncertainties about COVID-19 vaccines among Ugandan communities, and concerns that COVID-19 vaccines were developed rapidly, it is not surprising that there is a high level of skepticism on the vaccine among the study population.
With the unsuspecting and unforeseen side effects, it would be a balanced decision to weigh-in-the argument that it would not be wise to vaccinate children who have a longer life ahead-considering inadequate data on long-term effects of COVID-19 vaccines on Ugandan children.
However, a report from the Vaccine portal states that serious side effects that would cause long-term health problems are implausible following COVID-19 vaccination.26 It affirms that millions of children have received COVID-19 vaccines, and no long-term side effects have been detected.26 The portal assures that long-term side effects following any vaccination are infrequent, the COVID-19 vaccination inclusive.26 Historically, vaccine monitoring has shown that if side effects are to happen, they tend to happen within six weeks of a vaccine dose.26 Therefore, the Food and Drug Administration (FDA) ensured that each of the authorized COVID-19 vaccines had at least eight weeks of study after the final dose.26
In addition, the US CDC also reports that side effects after getting a COVID-19 vaccine vary from person to person, and they generally go away in a few days.27 Some people experience a little discomfort and can continue to go about their daily activities uninterrupted, while others have side effects that affect their ability to do daily activities.27
It further states that even if one does not experience any side effects, the body is building protection against the virus. In addition, the USA CDC confirms that adverse events after COVID-19 vaccinations are rare but can cause long-term health problems, occurring within six weeks of getting COVID-19 vaccines.27
However, we, the authors suggest that vaccination of Ugandan children with COVID-19 should be temporarily halted until sufficient data on long-term effects of COVID-19 vaccines have been determined in Ugandan children and parents have consented to the vaccination.
Study limitations
This was a one-off assessment of participants’ perceptions on COVID-19 vaccines. We, the authors, reckon that there may have been some social desirability biases that the research team could not control among research participants and, therefore, the need for more studies in the future, taking into consideration factors that may influence perceptions of participants. However, this study was conducted among a rural population using a face-to-face interview which enabled the research team to obtain up-to-date information from participants. The sampled population was large enough to get generalizable information on COVID-19 vaccines in the Acholi sub-region. Findings from this study should be interpreted in the context of a rural population that had just experienced a severe wave of COVID-19 in Uganda. We may not be sure that similar findings would have been obtained before the second wave or just after the first wave of COVID-19 in Uganda.
CONCLUSIONS
There were no substantial differences in perception on COVID-19 vaccines among adult age-group populations in northern Uganda. The determinants of COVID-19 vaccine perceptions were the importance of vaccines in protecting against the virus; vaccines have unlikely unforeseen side effects, and children could take the vaccine. Stratified by age-group populations and using age-group of less than 20 years as the reference category, the 20–29-year-old age-group and >50-year-old age-group perceived COVID-19 vaccines developed in Uganda as unlikely safe and effective; vaccines have likely unforeseen side effects and are unlikely being promoted for commercial gains. There is a need for health managers to continue engaging, sensitizing, and mobilizing the population by addressing concerns about the long-term and immediate side effects of COVID-19 vaccines.
Acknowledgments
We acknowledge, with many thanks, the financial support from UMA Acholi branch members, which enabled the team to conduct this study successfully, and the assistance from the administration of the twenty-four health facilities in northern Uganda.
Ethics approval and consent to participate
The study was approved by St. Mary’s Lacor Hospital Institutional and Ethics Committee (LHIREC No. 0192/10/2021). In addition, the study was conducted following relevant institutional guidelines and regulations.
Funding
All funds for this study were contributions from individual research members of the Uganda Medical Association (UMA) Acholi branch.
Authors’ contributions
DLK, ENI, JNO, JA, SB, LO, and FWDO designed the study. JA, JNO, PA, FWDO, and DLK supervised data collection. ENI, LO, JA, and DLK conducted data analysis and interpretation. SB, CO, PA, NOA, DA, JNO, DO, POO, SGO, FPP, ENI, FWDO, JA, LO, and DLK wrote and revised the manuscript. All Authors approved the final version of the manuscript.
Competing interests
All the authors completed the Unified Competing Interest form at http://www.icmje.org/disclosure-of-interest/ (available upon request from the corresponding author) and declare no conflicts of interest.
Availability of data and materials
All datasets supporting this article’s conclusion are within this article and are accessible by a reasonable request to the corresponding author.
Correspondence to:
David Lagoro Kitara
Takemi fellow, Harvard University
Faculty, Gulu University, Faculty of Medicine, Department of Surgery, P.0. Box 166, Gulu City, Uganda, email: [email protected]
(+256)772524474.