Hepatitis B virus (HBV) and hepatitis C virus (HCV) are major health problems and common causes of liver-associated morbidities.1 The World Health Organization (WHO) estimated that 257 million people are living with HBV worldwide2 and 71 million people are infected with HCV.3 HBV and HCV can cause acute and chronic infections, with the latter potentially progressing in severity at later stages and resulting in liver cirrhosis or liver cancer and eventually death. In 2015, HBV and HCV infections resulted in 887 000 and 399 000 deaths, respectively, most of which were related to either cirrhosis or hepatocellular carcinoma (HCC).4
Viral hepatitis is one of the leading causes of mortality and disability worldwide,5 putting those affected at risk of severe complications and lowering their quality of life, which may negatively affect their productivity. Some of its indirect burdens include lower productivity, increased absenteeism, and higher health care benefit costs.6
Oral antiviral agents are available for treating both chronic HBV and HCV, but the outcome and goals of treatment differ. For HBV, they include controlling the disease’s progression, preventing its complications, and achieving a functional cure. The required duration of treatment is still being discussed, especially regarding its completion. For HCV, progress in antiviral therapy means achieving a sustained viral response (SVR); novel genotypic drugs can achieve virologic cure in more than 90% of cases. However, patients who receive treatment and achieve a SVR must still be followed up routinely for liver disease progression, especially those who started treatment at an advanced stage of liver illness.7
Estimating the total cost of HBV and HCV infections is an essential health concern. Generally, viral hepatitis is linked with high health and economic burdens that affect policy decisions globally.7 In Lebanon, treatment for both HBV and HCV is available and provided for free to all Lebanese citizens through the Lebanese Ministry of Public Health (LMoPH). However, the cost of comprehensive treatment limits the ability of health care providers to acquire it, since it is associated with several expensive laboratory tests, including nucleic acid techniques, fibroscan, routine laboratory tests, and liver function tests.8 Several studies evaluated the cost of treatment and the management of hepatic and extra-hepatic complications. Evidence has shown that HBV can impose a substantial economic burden on patients, families, and communities.9 Similarly, HCV has been associated with extremely high costs and treatment expenditures.10 Rashid et al. showed that, as the HCV-infected population ages and the cost of treatment increases, the economic burden of chronic HCV infection grows proportionally, along with its clinical burden.11 Nasser et al. found that early HCV treatment is cost-effective compared to delayed therapy, emphasizing the need to reinforce early screening and linkage to care.12
Despite LMoPH’s commitment to treat all Lebanese affected with HBV and HCV, access to care is not always available in the country due to several economic and political factors. The limited budget available to LMoPH forced them to obtain generic treatments from neighbouring countries that are not always WHO-approved. The recent political crisis and the resulting socioeconomic collapse have further diminished the LMoPH’s ability to obtain necessary medications for chronic illnesses, including viral hepatitis. This has put many individuals at risk of forced interruption of their treatment courses and increased the risk of complications associated with chronic viral hepatitis.13
The Syrian crisis has further exacerbated this problem, as many Syrians sought refuge in Lebanon. Lebanon is currently believed to be the country with highest number of refugees per capita globally,14 which is heavily affecting the country’s health care system.15 With such drastic population mobility, a host country is expected to face numerous diseases and medical conditions, especially communicable diseases such as HBV and HCV.16 In fact, conflicts and war are often associated with the outbreak of serious infectious diseases.17–19 With Lebanon currently significant challenges, the problems associated with neglected infectious diseases must be addressed and rapid control measures should be established.
We aimed to assess the prevalence of HBV and HCV infections among the Lebanese and the Syrian refugees residing in Lebanon and comprehensively analyse the situation beyond a simple statistics-based approach. We also aimed to assess the risks associated with neglecting these infections among the refugee population and determine possible long-term consequences, while also suggesting possible interventions to address the aforementioned challenges.
METHODS
This is an observational cross-sectional study based on data from the LMoPH registry of communicable diseases. The Institutional Review Board (IRB) gave us approval to conduct this study and analyse the available data. We first obtained data on the prevalence of HBV and HCV infections from 2013 to 2018 among the Lebanese population and Syrian refugees residing in Lebanon, which we distributed based on age and gender. We then compared the prevalence of HBV and HCV among these two population with that of the Syrians still residing in Syria.
We sorted the data according to year, nationality, age, and gender and plotted it into tables and graphs. We conducted an extensive literature review via MEDLINE, Google Scholar, and PubMed utilizing the following keywords: refugees, Syrians, HCV, HBV, Lebanon. We analysed the data using the SPSS statistical software (IBM, New York, USA, version 25).
RESULTS
Lebanon
The population residing in Lebanon comprises the Lebanese people, Syrian refugees, Palestinian refugees, and other nationalities. Table 1 presents the prevalence of HBV and HCV infections and their distribution among the total population in Lebanon and the Syrian refugees residing in Lebanon from 2013 to 2018. In this period, 1701 HBV and 693 HCV cases were reported in Lebanon. On average, 283 HBV (range = 141-390) and 115 HCV (range = 102-136) cased occurred annually (141-390). The prevalence of HBV and HCV in Lebanon is 1.74% and 0.21% respectively, ranking Lebanon among countries with low endemicity for both viruses.20
From 2013 to 2018, 220 HBV cases and 40 HCV cases were among the Syrian refugees residing in Lebanon, amounting to an average of 37 HBV cases (range = 8-53) and 7 HCV cases (range = 4-10) per year. The HBV and HCV cases among the Syrian refugees accounted for 13% and 6% of all HBV and HCV infections diagnosed in Lebanon throughout the years 2013-2018.
The number of HBV and HCV cases was at its highest from 2013 to 2015, after which it stabilized and decreased over time (Table 1). Table 2 shows the distribution of the HBV and HCV cases in 2018 among the total population and the Syrian refugees in Lebanon, stratified by age and gender.
We then applied the estimated incidence rates (%) of HBV and HCV reported among Syrians in Syria to the Syrian refugees residing in Lebanon, to better approximate the true incidence the latter subgorup. The number of both HBV and HCV infections was significantly higher among the youth than other age groups for both populations. The 20-39 age group represented 40% of the HBV and 30% of the HCV cases among the total population. For the Syrian refugee subgroup, 57% of HBV cases and 28% of HCV cases were reported among individuals in the 20-39 age group. Adolescents and the paediatric population displayed the lowest prevalence for both HBV and HCV cases for the two populations. Only 2% of the total HBV cases and 5% of the total HCV cases among the total population in Lebanon were observed among individuals <19 years of age, while no HBV or HCV cases were recorded among the Syrian refugees in the same age group.
HBV and HCV were more prevalent among men than women for both the Lebanese population and the Syrian refugees. In 2018, 60% of HBV cases and 76% of the HCV cases in the total population residing in Lebanon were reported among men. Similarly, for the Syrian refugees, 75% of HBV cases were among Syrian males. The same trend was noted throughout all years from 2013 to 2018. The number of reported cases of HCV among female Syrian refugees was slightly higher than that among male Syrian refugees in 2018.
Syria
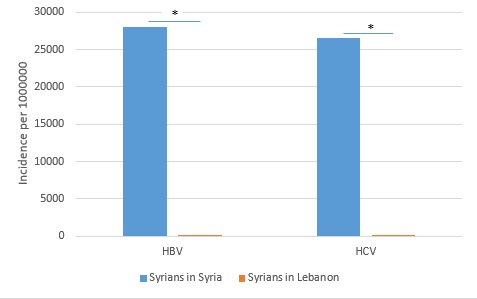
Among the total Syrian population in Syria, the prevalence of HBV and HCV was 5.6% and 2.8%, respectively, which is significantly higher than the prevalence among the Syrian refugees in Lebanon for both HBV and HCV.21 The comparison between the incidence rates (per 1 million) of HBV and HCV among the Syrians in Syria and Syrians residing in Lebanon is presented in Figure 1.

We then applied the estimated incidence rates (%) of HBV and HCV among Syrians in Syria to the Syrian refugees residing in Lebanon to better approximate the true incidence among the latter subgroup. We calculated the expected number of HBV and HCV cases based on the total number of registered Syrian refugees in Lebanon (n = 948 849). The number of HBV and HCV cases recorded among the Syrian refugees in Lebanon was significantly lower than the calculated number of HBV (n = 53 135) and HCV cases (n = 26 567) (Table 3).
DISCUSSION
We found a notable difference in the prevalence of viral hepatitis between the Syrian refugees in Lebanon and the Syrians residing in Syria. Viral hepatitis is a global health threat and a worldwide development priority.22 The global burden of HBV and HCV is a growing issue and is most challenging in areas of conflict. War, displacement, and political crises are often associated with the outbreak of infectious diseases, especially as asylum seekers are at a higher risk of transmissible infections.19 Refugees constitute a special social group in a geographical area and are often forced to live under conditions that facilitate the spread of infectious diseases. Moreover, the prevalence of chronic infections among them depends on the endemicity of these diseases in the country of origin.23
The Syrian conflict, which started in 2012, disrupted the lives of many Syrians, many of whom sought refuge in nearby Lebanon, which exacerbates its ongoing political, economic, and social crises. Lebanon’s infrastructure, economy and health care sector was excessively overburdened and limited resources were available to its fast-growing population.24
In Lebanon, the prevalence of HBV has decreased after the implementation of several interventions, including HBV vaccination of newborns since 1998, the implementation of mandatory premarital screening implemented since 1994, and the establishment of different awareness campaigns.25 However, the high number of refugees and catastrophic political and economic events have negatively impacted the country’s public health system, and consequently, its efforts at containing viral hepatitis infections. Here we assessed the prevalence of HBV and HCV among the Syrian refugees in Lebanon with reference to the prevalence among the total population in Lebanon from 2013 to 2018. According to LMoPH’s registry of communicable diseases, 13% of all HBV and 6% of all HCV cases in the country were among the Syrian refugees. The incidence rates of HBV and HCV among the Syrians in Lebanon was significantly lower than among the Syrians remaining in Syria. To deepen these findings, we conducted further exploratory analyses
Table 3 shows the expected numbers of HBV and HCV cases among the Syrian refugees residing in Lebanon based on the incidence rates (%) of HBV and HCV reported among Syrians in Syria applied to the Syrian refugees residing in Lebanon. There is a marked discrepancy with the numbers reported to the LMoPH, implying that the true number of Syrian refugees infected with HBV or HCV is much larger. This raises significant concerns and may indicate that the HBV and HCV cases are being underreported or underdiagnosed. It may also indicate insufficient disease surveillance activity in Lebanon. Moreover, the true number of Syrian refugees in is likely much higher than our estimates, as many of them are not registered; this would mean that the extrapolated prevalence is much lower and that issue of underreporting more drastic. The diagnosis and reporting of communicable diseases are important steps for evaluating and constructing disease control programs and are valuable for overall disease surveillance. Surveillance itself is an essential tool for identifying new outbreaks and trends and monitoring the progression of certain diseases.26 The absence of either of these interlinked components can prevent proper epidemiological assessments and result in detrimental health outcomes. For example, HCV surveillance has poor sensitivity27 due to under-detection and under-reporting. Under-detection has mainly been attributed to the disease’s slow, silent onset,28 while under-reporting has been shown as the result of political turmoil, indifference, and poor infrastructures.29 HCV attack-rates are systematically underestimated due to the insensitivity of HCV surveillance,30 especially if surveillance focuses only on acute infections, which are rarely symptomatic. According to the WHO, since patients will not realize they are infected, screening is recommended for the entire population in countries with high prevalence. However, this is rarely applied.
Two hypotheses are proposed for the current HBV and HCV findings: linkage to care and the principle of neglected diseases. Linkage to care is crucial for dealing with terminal infectious diseases, including viral hepatitis. Once tested, patients who are linked to care can achieve significant reductions in HBV-associated morbidity and mortality.31 Lok et al. noted that linking HBV-infected patients to care facilitates timely treatment for eligible persons and allows for the periodic surveillance of HCC and monitoring of disease progression.32 Coyle at al. indicated that linkage to care can enhance HCV care continuum and allow for the establishment of behavioural risk reduction counselling, as well as the vaccination of susceptible contacts.33 In Lebanon, several factors can influence linkage to care. Individuals may be unaware of their infection or unreferred to a specialists, despite their diagnosis.34 Lack of effective screening policies, poor health literacy, and high cost of treatment and follow-up expenses may also prevent any attempts towards linkage to care.35 Non-existence of linkage to care can impose individual and national financial burdens and can make the eradication of the disease less feasible.
The second principle is related to neglected diseases, which are common among populations with lower income and socioeconomic status, who do not present an attractive or profitable market for stakeholders in the private sector when it comes to research and drug design.36 Constantly burdened by underdevelopment, poverty, and health inequity, these populations are susceptible to HIV/AIDS, malaria, tuberculosis, and a multitude of neglected diseases.37 The global focus on the first three diseases overshadows the sufferings that neglected diseases, often overlooked by media and governments, are causing to millions of people. This results in a lack of awareness of the diseases’ symptoms and complications, as well as the importance of screening and the implementation of reporting and surveillance strategies.38 Lebanon is a country of low HBV and HCV endemicity and these infections are not considered major priorities, which is why Hepatitis B and C have become neglected diseases.
This implies that the Syrian refugees in Lebanon are subject to a cumulative risk of complications in the absence of proper screening and treatment. HBV and HCV progressions are often silent and many patients remain unaware of their infection until later stages of cirrhosis, liver decompensation, or HCC.39,40 Reports show that 55%-85% of people with acute HBV develop chronic infection and about one third, if not treated, eventually develop liver cirrhosis or HCC.41 Furthermore, it has been shown that the five–year cumulative risk for HCC was 9.7% to 15.5% in cirrhotic patients.42 Most patients infected with HCV have different degrees of liver damage that can worsen, leading to liver cirrhosis in 20% of the cases.43 One-third of patients with predominantly mild HCV showed significant fibrosis progression over a median period of 30 months.44 However, individual variability is wide, and it is not yet possible to predict who will progress to more severe states or in what period. The HCV disease paradigm varies by country based on historical and present risk factors, screening programs, and treatment methods.45
In developing countries with the highest prevalence of HBV and HCV, treatment capacity and financial resources are limited. Screening and treatment are prioritized for patients in more advanced stages of the disease,46 which prevents the early identification of cases. According to the WHO, early identification of HBV and HCV cases enables linkage to care and prevention or delay of progression of liver diseases. It also allows the reduction of transmission through counselling and vaccination.38 Even though the overall prevalence of viral hepatitis is expected to decrease over time, the morbidity and mortality attributed to viral hepatitis are expected to increase as the presently infected population progresses to advanced stages of liver disease.47 For instance, under the current treatment paradigm, the prevalence of chronic HCV is projected to decrease by 4% by 2030, but cases of advanced stage liver disease are projected to increase by 18%-30%.48 Sibley et al. found that the number of HCC cases attributable to HCV was projected to increase by 25% by 2030 from a base of 30 cases and that compensated cirrhosis and decompensated cirrhosis were also projected to increase by 30% and 17%, respectively, from a base of 810 and 90 cases in 2014.47 This implies that the cumulative risk of chronic complications is continuously rising. Further neglect of such infections can impose severe burdens especially for struggling countries.49
Lebanon is currently struggling with financial and political instabilities which significantly impacted its already overburdened health sector. Given the expected progression of these infections, thorough assessments and careful measures are needed to better control HBV and HCV and their long-term sequelae.
According to the data presented in Table 2, 60% of HBV cases and 76% of HCV cases in 2018 in the total population residing in Lebanon corresponding occurred among the 20-39 age group. Several studies have shown that HBV and HCV disease progression is an age-dependent process, as it has been shown to be a strong determinant of chronicity at the time of infection. The earlier the acquisition of infection, the higher probability of developing chronic infection.50 The National Health and Nutrition Examination Survey (NHANES) study on HCV infection estimated the chronicity rate at 30% in subjects below under 20 years of age, and 76% for those over 20 years.51 Also, Pradat et al. showed that most HCV patients, if untreated, are expected to develop cirrhosis at about 65 years, irrespective of the age at infection.52 This raises several concerns for Lebanon, where the relatively young Syrian refugee population is currently aging while waiting for the resolution of the Syrian conflict. This implies that the burden of HBV and HCV chronicity will be more pronounced in the future. Thus, it is important to highlight the cumulative risk assessment associated with viral hepatitis. The lack of patient identification protocols and efficient screening strategies prevents any opportunities for clinical interventions before the onset of severe liver complications, further exacerbating this burden, which is expected to be increase as Lebanon’s health care capacity continues to diminish. Efforts should be targeted towards enhancing the linkage to care process in Lebanon.
We also found higher HBV and HCV prevalence among men than women in both studied populations. This is in accordance with previous literature indicating that the rate of chronicity for HBV and HCV infections appears to be lower in women, particularly younger women.53,54 Such conclusions are essential for the prioritization and elimination strategies of viral hepatitis particularly in a limited resources setting such as Lebanon.
Despite being neglected diseases, some efforts have focused on the elimination of HBV and HCV. The WHO has recently issued its first guidance for country validation of HBV and HCV elimination and provided recommendations for screening, care, and treatment of persons with chronic infections.55 Newly developed drugs have revolutionized treatment of HBV and HCV compared to traditional drugs and have exhibited great efficacy, high tolerance, and minimal side effects.56 However, despite these advancements, the eradication of viral hepatitis remains to be unattainable in Lebanon,11 which, like many low- and middle-income countries, struggles with a lack of awareness among patients, high costs, and shortages in medicines and care utilities.45 Although the price of medicines effective against HBV infection have decreased sharply, Hutin et al. found that there is significant underutilization of low-price, generic medicines effective against HBV.57
Such challenges are more significant considering the high number of refugees in Lebanon. Refugees are an underprivileged population which often experiences unstable living conditions and is expected to exhibit elevated rates of HBV and HCV.58 United Nations High Commissioner for Refugees (UNHCR) provides certain medical services to the Syrian refugees in Lebanon, including vaccinations, medications for acute illnesses, two ultrasounds for pregnant women, and discounts varying from 10%-15% on some other services. Among these services, only vaccination against HBV is offered as part of routine children vaccination program.59 Findings have shown that Syrian refugees spend only 12% of their income on medical expenses,60 which presents an additional burden alongside their existing financial struggles in their host country. This makes them reluctant towards seeking diagnosis and linkage to care and further pressures the overloaded Lebanese health care sector that is experiencing shortages in medical resources. This pressure results in disparities in the distribution of health care services and treatments. Consequently, ethical dilemmas arise regarding the prioritization of these treatments among the refugees and host population.61,62 These issues should be addressed to decrease the social and economic burden on the Lebanese government and its people.
Action is needed to prevent further neglect of HBV and HCV. Early steps towards eradication and decreasing the expected cumulative burden are crucial. This can be achieved through outreach campaigns to ensure community awareness and to promote a better understanding of HBV and HCV. Efficient proactive screening based on risk analysis is needed. The Lebanese government must establish a responsive, people-oriented health care system and ensure access to affordable diagnostics and treatments. Imaging modalities required for early HCC such as magnetic resonance imaging (MRI) and computed tomography (CT) scans should be provided with minimal costs. This will allow systematic surveillance and regular reporting and will enhance testing and linkage to care.
Limitations
This study has some limitations. The number of Syrian refugees included in this study is not representative of the true number of refugees, which expected to be higher, so our sample is not representative for the whole population. We also did not assess the risk of the “health migrant” effect. Furthermore, this study focused on the number of confirmed HBV and HCV cases, but did not cover the number of cases with severe liver complications.
CONCLUSION
Hepatitis B and C are neglected diseases in the Syrian refugee population. This continued neglect will render this vulnerable population at a higher risk of chronic viral hepatitis complications and mortality, further increasing the health and economic burden in a country already financially strained. Urgent action is needed by the host country and by the international community to apply better surveillance, detection and linkage to medical care. Given the limited resources available for the Lebanese government, international organizations involved in the health of Syrian refugees should prioritize the management and prevention of viral hepatitis B and C in Lebanon.
Ethical approval
An approval from the Institutional Review Board (IRB) was not needed for conducting this study.
Funding
No funding was used to complete this manuscript.
Authorship contributions
Abdul Rahman Bizri and Laya Al Mahmasani had access to data collected for the study. Layal Al Mahmasani and Zeina Bayram contributed to data analysis and manuscript writing. Abdul Rahman Bizri was responsible for the design and supervision of the study. Umayya Musharrafieh assisted in the study design. All authors read and approved the final version of the manuscript.
Disclosure of interest
The authors completed the ICMJE Disclosure of Interest Form (available upon request from the corresponding author) and disclose no relevant interests.
Correspondence to:
Zeina Bayram
American University of Beirut
Beirut 1107 2021, Lebanon
[email protected]