In 2021, 38.4 million people globally were living with human immunodeficiency virus (HIV), and 1.5 million people became newly infected with HIV, of which 70% were key populations and their sexual partners.1 Key risk groups include sex workers, people who inject drugs, prisoners, transgender people, and men who have sex with men (MSM) at high risk and burden of HIV infection.2 HIV testing with counselling and linkage to care service is critical to engaging key populations in HIV care; however, they face barriers to accessing such services due to fear of experiencing stigma and discrimination.2 In 2016, World Health Organization (WHO) added HIV self-testing (HIVST) to its recommended testing approaches, aiming to reach key populations and people who may not test otherwise.3 HIVST is a process in which a person collects his or her specimen and then performs an HIV test and interprets the result, often in a private setting, either alone or with someone he or she trusts.3 HIVST is effective in scaling up HIV testing uptake among key populations due to its cost-effective, confidential, and convenient features.3 However, lacking linkage to care is reported as a key challenge in HIVST, and there is a concern that HIVST without counselling support and timely linkage service could lead to missing or delayed initiation to treatment.3–7 In the routine HIV testing context, linkage to care is defined as patient entry into specialist HIV care after diagnosis, measured as the time between the HIV diagnosis date and one of the following markers: either the first clinic attendance date, first CD4+ cell count or viral load date, or HIV treatment start date, depending on data availability and linkage is considered prompt if within three months of diagnosis.8 However, following a positive HIVST result, confirmatory testing is needed since a positive HIVST result alone could not diagnose HIV. For those with negative HIVST results, linkage to relevant prevention is necessary since key populations are at ongoing high risk and must be regularly retested.4 Currently, key populations’ care-seeking behaviour patterns following HIVST and the linkage approach are unknown, and there is no comprehensive guideline on linkage to care for key populations after HIVST. It is noticed that recent HIVST studies and reviews have addressed the concern of the inadequate linkge to care after HIVST and explored various implementation strategies to promote linkage to care, for instance, the innovative digital-supported HIVST (e.g., website-based, social media, mobile applications (apps)), which showed promising results in various settings.9–11 The emerging published evidence and ongoing clinical trials make it necessary to identify and summarise the current linkage-to-care promoting strategies to inform future HIVST research and implementation. Therefore, this scoping review aimed to identify and synthesise the current global evidence on the implementation strategies to promote linkage to care for key populations after HIVST.
METHODS
This scoping review was conducted following the Joanna Briggs Institute Manual for Evidence Synthesis (Chapter 11: scoping reviews).12 The report of this scoping review referred to the Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) checklist.
Eligibility criteria
The eligibility criteria for included studies were decided based on the Population, Concept, Context (PCC) framework proposed by Peters et al.12 The PCC framework is appropriate for scoping reviews because it allows for the inclusion of studies that do not contain information about outcomes or comparator groups. Eligible populations included sex workers, MSM, people who inject drugs, prisoners and transgender people. Studies addressed the concept of HIVST and linkage to care were included. There was no limitation on the study context. Specifically, studies that fulfilled the following criteria were included for review: 1) involved key populations; 2) described the HIVST approach; 3) reported implementation strategies to facilitate linkage to care; 4) reported linkage outcomes or measurements. This scoping review considered the following studies for inclusion: randomised controlled trials, non-randomised controlled trials, cohort studies, descriptive observational studies, and implementation studies. Ongoing clinical trials or study protocols that met the inclusion criteria were also eligible for inclusion. Qualitative studies, review articles, opinion papers, and conference abstracts were excluded.
Search strategy
The search strategy was developed by consulting a professional librarian and was modified and applied for use in the following databases: PubMed, Embase, EBSCOhost, Cochrane Library, Wan Fang Data (Chinese), China National Knowledge Infrastructure (Chinese), and Japan Medical Abstracts Society (Japanese). Search terms involved Medical Subject Headings (MeSH) and were combined using the Boolean operators’ AND’ and ‘OR’. There was no restriction on language or published date; however, we only included articles written in English, Chinese, or Japanese. Search queries and results for each database are documented in Appendix A.
Study selection
All the initially identified articles from the database search were exported to Rayyan (Qatar Foundation, Al Rayyan, Qatar)—a free web and mobile app that expedites the initial screening of abstracts and titles.13 After removing duplicates, title and abstract screening was conducted by three independent reviewers (PM, RS, XS) to make sure each article was double-checked. After the title and abstract screening, the remaining articles were subject to full-text screening for eligibility based on the inclusion criteria. Disagreements on article eligibility were resolved through consensus among the three reviewers.
Data extraction and presentation
A data extraction tabular form was used to abstract and record the data from the eligible articles. The first author conducted the initiative data extraction, and the second author double-checked the entered data to ensure completeness and accuracy. Data extraction modules included author, published year, country, study population, study design, implementation strategy to promote linkage to care, and linkage outcome and measurement. Results of implementation strategies to promote linkage to care after HIVST were analysed and classified thematically and presented in a narrative synthesis.
Ethics consideration
Given that this scoping review used publicly available literature, the requirement for ethical approval was waived.
RESULTS
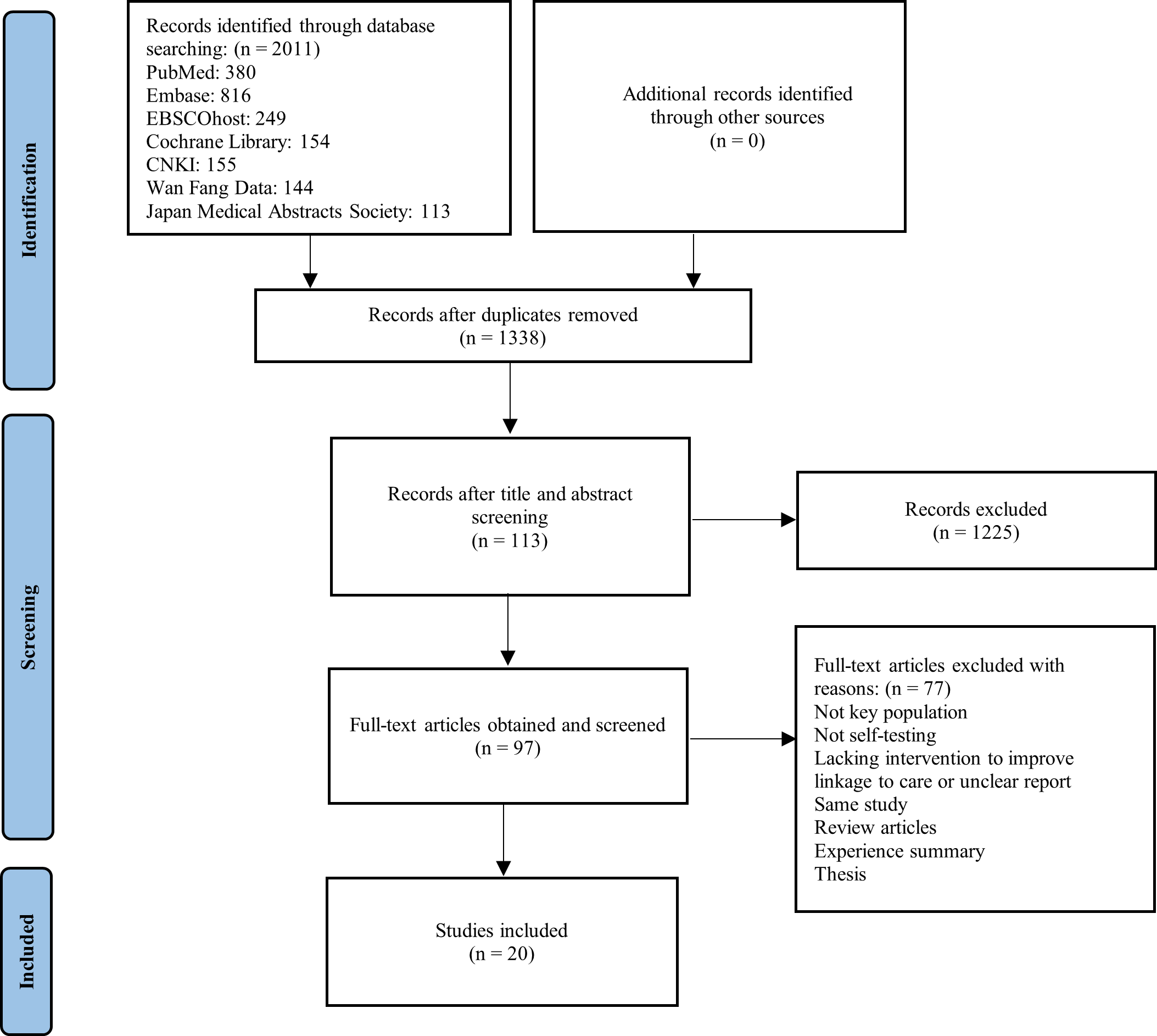
The results of the database searches yielded 2011 articles. After removing duplicate articles, 1338 articles remained and were subjected to title and abstract screening. After the completion of title and abstract screening, 113 articles remained, and 97 full-text articles were retrieved and further subjected to full-text screening. Finally, 20 studies met the eligibility criteria and were included in the review. Figure 1 shows the study selection process from a database search to screening and the final selection of included studies.

Characteristics of included studies
The 20 included studies were categorised into implementation studies (10), randomised controlled trials (8), cohort studies (1), and cross-sectional studies (1). Nine studies targeted MSM, seven focused on the mixed population, including MSM, transgender people, people who injected drugs, and other high-risk populations, three studies on female sex workers (FSW), and one on transgender youth. In terms of time and setting, six studies were in the US; seven studies were from Asia: China (3), Vietnam (2), Thailand (1), Iran (1); five studies in Africa: Kenya (2), Nigeria (1), Uganda (1), Zambia (1); one in the UK and one in Canada. The in-depth findings from the included studies are summarised in Table 1.
Implementation strategies to promote linkage to care for key populations after HIVST
Seven categories of implementation strategies to promote linkage to care for key populations after HIVST were identified: 1) HIVST kits with linkage-to-care information, 2) web-based or mobile app-guided HIVST, 3) remote HIVST counselling, 4) intensive follow-up, 5) HIVST through social media and key opinion leaders, 6) community-based HIVST and 7) financial incentive.
HIVST kits with linkage-to-care information.
Providing HIVST kits with linkage-to-care information could be the initial step to promote linkage to care after HIVST, although management of cases with positive result and follow up remained as important challenges.14,15 In the US, vending machines were used to distribute test kits in commercial sex venues, and the test kits were attached with information about medical assistance and the Linkage-to-Care Hotline in case of a reactive test result.14 Among 17 initial positive HIV results, seven sought confirmatory testing, four initiated treatment, and two were linked to care.14
Web-based or mobile app-guided HIVST
The web-based or mobile app-guided HIVST program provided a digital toolkit for key populations to perform self-testing, interpret test results correctly, and get rapidly linked to and stay in care.9,16,22,23 In the SELPHI study protocol,16 the study website was designed to direct participants with a reactive HIV test result to local genitourinary medicine clinics and HIV care services. The SMARTtest project9 used a smartphone app to instruct HIV self- and partner-testing and gained positive feedback from participants regarding the video display, step-by-step instructions, and the testing results sharing features. This study noted participants’ preference for LGBT-friendly clinics versus a list of all available resources for linkage to care referral services on the smartphone app.9
Remote HIVST counselling
Remote HIV counselling via telephone or video-chat platforms allows health personnel to provide self-testing and results-interpreting instruction, risk management, and linkage support to participants in a direct and timely manner.17–21 In the US, Wray et al.21 developed an eTest system to notify researchers to schedule post-test phone counselling within 24 hours after users initiated HIVST. Another project—Moxie18 in the US, proposed using video-based HIVST counselling to provide risk elicitation and identification interview, guidance on self-testing, result reading, prevention plan and linkage direction to participants. In a pilot project in China,20 all the four users who received positive HIVST results after HIVST online counselling received immediate support and were linked to care and treatment. However, in Thailand,19 participants who self-selected the online-supervised HIVST and counselling turned out to have poor linkage to pre-exposure prophylaxis (PrEP) services (10.2%), low HIV confirmatory testing rate (75%), and low antiretroviral therapy (ART) initiation rate (52.8%) compared with the routine HIV testing group.
Intensive follow-up
Intensive follow-up through text messages and phone calls was necessary when participants whom self-tested positive needed to be reminded and pushed to attend HIV care.18,19,25 In the project Moxie, for participants who received reactive testing results after the video-based supervised HIV self-testing and counselling, follow-up was scheduled on the following day, and each participant was to be contacted at least three more times to ensure a medical appointment was attended, and a confirmatory test result was reported.18 In Nigeria, Tun et al.25 distributed oral HIVST kits to MSM through key opinion leaders and achieved complete linkage with active follow-up and access to a trusted MSM-friendly community clinic that offers HIV treatment. However, Phanuphak et al.19 study from Thailand, despite referred participants in the online HIVST and counselling group being followed up on day 3, weeks 1, 2, and every two to four weeks, the ART initiation rate was only 52.8% (19/38). This study found that MSM and TGW who selected the online group were more likely to fear meeting people they might know when getting HIV testing and were more likely to experience discrimination within families due to gender identity than those who opted for routine testing.19
HIVST promotion through social media and key opinion leaders
The social media and key opinion leaders (KOLs) strategy was an economical and efficient way to reach key populations and increase HIV identification and link-to-care.25–27 In Nigeria, HIVST kits were distributed to MSM by influential KOLs self-identified as MSM or gay, had good interpersonal skills, and had real-time information about their MSM community and hotspots.25 In Vietnam, Green et al.26 led an HIVST promotional campaign using Facebook, Grindr, and MTV for MSM to connect and exchange information on HIV, sexuality, and wellbeing, and they trained social network influencers to communicate with Rainbow Village followers to provide HIV risk screenings and referrals for HIV testing. A national pragmatic study in China engaged six social media KOLs located in 4 provinces and one city to advertise HIVST programs on social network platforms, which enabled the researchers to recruit MSM from 30 provinces and cities simultaneously without being restricted by regional barriers.27 The authors concluded that HIVST via the social media KOL strategy yielded lower recruitment costs, HIV testing costs, and HIV-identified costs but a lower incidence of HIV than the community-based organisations-led HIVST approach.27
Community engagement in HIVST: community-based organisations-led HIVST; peer-engaged approach; partner notification service
Two HIVST studies in Vietnam26 and China27 engaged MSM Community-Based Organisations (CBOs) and demonstrated the active role and significant public health impact of CBOs-led outreach and follow-up services for key populations. In the CBOs-led HIV lay testing and self-testing program in Vietnam, staff from MSM CBOs were trained to offer HIV testing information and support MSM with HIV-reactive results for confirmatory testing and ART enrolment.26 In Zhang et al.'s study, MSM CBOs staff posted HIVST advertisements through social media and offline events to recruit MSM, and trained volunteers from local CBOs paired up with local health departments to help participants with positive self-testing results to take confirmatory testing and treatment.27
Four studies conducted in Zambia,28 Uganda,29 Kenya,30 and Vietnam31 used a peer-engaged approach and partner notification service in their community-based HIVST programs. Chanda et al.28 and Ortblad et al.29 trained FSW peer educators who were trusted and respected within the local FSW community to distribute oral HIVST kits, give HIV risk reduction counselling and education on self-test use, results interpretation, and linkage to care. In Kenya,30 peer mobilisers distributed HIV self-test kits within their networks and immediately referred clients with acute and early HIV infection symptoms to HIV testing. Furthermore, the mobilised participants with HIV infection were encouraged to invite their partners to HIV testing through the partner notification service.30 The authors noted that the partner notification service was effective in HIV case-finding and identifying acute and early HIV infection among partners of high-risk populations.30,31
Financial incentive
In China, Zhang et al.27 and Zhong et al.24 integrated a financial incentive strategy using online payment into their studies to facilitate linkage to care for MSM after HIVST. Zhang et al.27 required a deposit of $7.25 for an HIVST kit and returned the deposit once the participant completed the online questionnaire and uploaded the test result, and the $7.25 deposit was rewarded to CBO staff if they successfully linked per HIV-infected individual to ART. Similarly, in Zhong et al.,24 social entrepreneurship model, MSM participants bought the HIVST kits for $23 and got refunded after successfully performing the HIVST and reporting the results. In Iran, Mirzazadeh32 registered an RCT-designed clinical trial to verify the effect of monetary incentives on HIVST uptake and linkage to care among female sex workers, their clients, and partners.
DISCUSSION
This scoping review summarised seven categories of implementation strategies to promote linkage to care for key populations after HIVST: 1) HIVST kits with linkage-to-care information, 2) web-based or mobile app-guided HIVST, 3) remote HIVST counselling, 4) intensive follow-up, 5) HIVST promotion through social media and KOLs, 6) community engagement in HIVST and 7) financial incentive.
Providing linkage information along with the test kit is essential and highly practical, and it could be the initial effort to promote linkage to care in HIVST programs. Web-based or mobile app-guided HIVST offers a comprehensive toolkit to guide self-testing, results interpreting and linkage to care. Remote HIVST counselling allows health providers to interact with participants directly, monitor their results, and tailor individual care plans timely, which addresses the concern that lacking counselling in HIVST leads to missing or delayed initiation to treatment.7,29 Intensive follow-up is necessary when HIV-reactive test users delay seeking confirmatory testing and treatment. However, caution should be taken as repeated follow-up could be perceived as being against client autonomy and thus deter HIVST utilisation.33 The use of social media and KOLs is an efficient and cost-effective strategy to promote HIVST and care information among key populations. Community-based HIVST, including CBOs-led delivery and follow-up, peer-engaged approach and partner notification service, can reach hard-to-reach and higher-risk populations, which is an important pathway for HIV prevention, testing, and treatment in some low- and middle-income countries where CBOs are highly involved in HIV care.34 Financial incentives can help improve the uptake of HIV testing, ART adherence, and continuity of care,35 but misuse of incentives and the requirement of participants to receive the incentive in person may appear as challenges in HIVST programs in resource-restrained settings.36,37
It is noticed that most HIVST programs strived to maximise linkage to care through multiple levels of efforts, such as remote HIVST counselling with intensive follow-up18 and HIVST promotion by social media KOLs and CBOs staff with a financial incentive.27 Indeed, no single implementation strategy could ensure full linkage to care after HIVST since multiple factors at the individual level, health provider level, and system level could influence linkage outcomes for key populations.38 Therefore, researchers and HIVST programmers should carefully assess the contextual and individual factors that affect care linkage for key populations and incorporate linkage services accordingly and effectively to ensure successful linkage after HIVST. Moreover, since stigma and discrimination remain major barriers for high-risk populations to take HIV testing and treatment,38,39 linkage services for key populations should be delivered discreetly and safely, without breaking the confidential and convenient nature of HIVST.
Although the evaluation of the linkage-to-care outcome was not a focus of this scoping review, we noticed a high heterogeneity in the measurement of linkage outcomes for key populations following HIVST. Most studies didn’t clarify the linkage time, while studies reported linkage time using different observation periods. A few studies on MSM and transgender people included PrEP as part of the linkage service,21,23,30 while most studies didn’t involve PrEP service. These findings agree with previous studies reporting that a mixed metric of effectiveness made it difficult to assess the linkage outcome of HIVST studies.10,33 According to Choko et al.,33 measuring linkage at the individual level following HIVST was resource-intensive, challenging, not feasible, and undesirable in some low-income settings where scaling up of HIVST was the priority and pragmatic and innovative ways to measure linkage following HIVST should be developed. To date, there is no standardised definition or unified measurement of linkage to care after HIVST.10 Given that HIVST is a different approach compared with facility-based HIV testing, the concept and definition of linkage to care following HIVST and indicators to measure linkage outcomes should be differentiated and standardised to guide future HIVST research and practice.10
In this scoping review, six of eight RCT studies were study protocols or registered clinical trials, and five centred on digital-supported interventions, mainly for MSM in high-income settings. This finding is in congruence with a previous systematic review reporting that data on digitally supported HIVST interventions in low- and middle-income countries were limited due to resource constraints and technology barriers.10 Another group of key population—female sex workers, who are at 30 times greater risk of acquiring HIV than the general female population and are burdened with structural and societal stigma, discrimination, and significant inequalities,40 may have different needs and preferences as end users of the digital-supported HIVST. Thus, it is warranted that future HIVST studies establish the evidence regarding the effectiveness of the digital-supported intervention on linkage to care for FSWs and high-risk populations in low and middle-income settings.
Limitations
Although this scoping review managed to systematically summarise a variety of implementation strategies that showed promising potential to promote linkage to care for key populations after HIVST, some limitations should be considered. Firstly, the search resources and language may restrict us from reaching a broader scope of the latest relevant studies. The studied populations were mainly MSM and TGW, which could limit the generalisation of the evidence to FSWs and other key population groups. Secondly, in most HIVST studies, linkage to care was not studied as a primary outcome, and some included studies were research protocols and registered clinical trials. This limited our interpretation of those implementation strategies’ effect and impact on linkage to care outcomes. Thirdly, the lack of quality appraisal of the included studies could limit the evidence quality and implications for practice.
CONCLUSIONS
Implementation strategies to promote linkage to care for key populations are diverse and should be incorporated in different settings and backgrounds. Innovative digital-supported HIVST research for female sex workers and high-risk populations in low and middle-income settings is warranted. A standardised definition of linkage to care following HIVST and a unified measurement of linkage outcomes should be developed and applied in future research.
Acknowledgements
We would like to express our appreciation to Prof. Honghong Wang from Central South University, China, for her insightful instructions and advice on this work.
Funding
This work is supported by the Japan Agency for Medical Research and Development (22rea522103h0001).
Authorship contributions
All authors contributed to the development of the review question and review strategy. PM, RS, and XS contributed to data collection and data extraction. EO provided instructions and supervised the review work. PM drafted the manuscript. RS and XS provided critical feedback and revision of the manuscript. All the authors have read and approved the final manuscript.
Competing interests
The authors completed the Unified Competing Interest form at http://www.icmje.org/disclosure-of-interest/ (available upon request from the corresponding author) and declare no conflicts of interest.
Correspondence to:
Panpan Ma, Department of Global Health Nursing, St. Luke’s International University, Tokyo, Japan.
[email protected]