
The emerging ethical concerns surrounding the short-term medical mission (STMM) model have been explored extensively in the literature.1–5 These concerns include a lack of sustainability and local partnerships, inadequate cultural preparation and pre-departure training, poor adherence to clinical best practices and medical providers practising outside their scope.5 Such deficiencies can potentially expose patients to inadequate care, negatively impact the healthcare system in fragile economies and contribute to dependency. These criticisms of STMMs have led to increasing calls for regulation and even the cessation of poorly structured humanitarian efforts.
Previously, these headwinds took place in the context of a trend towards increasing globalisation and increased travel. Although poorly described and constantly changing, the number of STMMs was assumed to be vast and growing, consuming substantial financial resources and involving an organisational landscape that is constantly in flux.4,6 Well-meaning healthcare professionals were faced with the prospect of selecting an STMM experience that they could not correctly vet, which would have an uncertain impact on the recipients of their efforts in host communities.
The landscape of such STMMs was radically altered by the COVID-19 pandemic, in which travel restrictions, quarantine requirements, and challenges to financing and charitable funding disrupted an already tenuous balance.7 These unprecedented obstacles forced an obligatory pause during which most STMM-sending organisations had an opportunity to reassess their efforts or, in some situations, faced an insurmountable barrier to continuing their programs.
The region encompassing Latin America and the Caribbean (LAC) is the most common destination for North American volunteers,8 and the impact of COVID-19 on both these continents was devastating. In this context, it remains unclear to what extent STMMs based in North America were disrupted, what contingency plans were set in place for host communities, and when and if organizations have plans to restart their efforts or modify their objectives.
Potential pandemic-related pivots may have prioritised training (either in-person or virtual) and education over direct service, sending equipment rather than people, or sponsoring the education or practice of local healthcare professionals working in underserved communities. Some sending organisations successfully implemented virtual programs or continued socially distanced versions of their nutrition programs.9 Others diverted funding towards providing medical supplies and personal protective equipment for clinic teams and sent emergency food kits in recognition of increasing food insecurity caused by pandemic restrictions.10 The scope and extent of these changes are unclear, but describing the phenomenon is important to understanding the trajectory of global health interventions in a potential “new normal” of reduced travel, increased restrictions, and financial uncertainty.
The primary objective of this study was to describe the perceived effects of the COVID-19 pandemic on STMMs serving LAC in terms of attitudes, funding challenges, adoption of alternative models of care, and plans for future humanitarian deployments.
METHODS
A multiphase methodology was used to longitudinally follow up with STMMs operating in LAC in 2014-2015 and to provide quantitative and qualitative descriptions of pandemic-related changes in their programs.
Sampling of STMMs
The sample for this study consisted of the 359 organisations found in the Medical Service Trip database, the largest online database of primary care STMMs operating in LAC at the time of its creation. The original database can be found at http://medicalservicetrip.com, and a map of the geographic distribution of the sending organisations is shown in Figure 1.

Sending organisations operating STMMs in LAC were sampled and identified in three ways in 2014-2015. First, several online databases were used (www.missionfinder.org, www.medicalmissions.org, www.mmex.org, www.globalhealth.arizona.edu, www.internationalhealthvolunteers.org) to identify STMMs. Second, based on a similar search for short-term STMMs conducted by Lasker,3 a systematic Google web search was conducted every two months between April 17, 2014 and July 20, 2015 using the following terms: “medical missions”, “short-term missions”, “medical mission organisations”, “international health volunteering”, “Christian health volunteering”, “religious health volunteering”, “corporate global health volunteering”, “international health fellowships”, “international health educational opportunities”, “global health director”, “international service learning”, “global health elective”, “medical school international internships”, “intercultural learning”, “global health volunteer projects university” and “international volunteer organisations”. Third, organisations were located through social media, using the Twitter hashtags “medical mission” and “global health”.
Organisations were included if they: facilitated North American clinicians (physician, physician assistant, osteopath, or nurse practitioner) travelling to LAC to provide direct care and had operated at least one short-term (i.e., less than one month) primary care medical mission in the previous year. Organisations were excluded if they exclusively performed specialty or surgical trips or conducted trips that did not involve direct patient care by North American clinicians.
We extracted the following information from each organisational website: the country/countries served in LAC (Figure 1), the location of their headquarters in North America, type of organisation (faith-based, secular, or educational), type of clinic (mobile, standing, hospital-based), trip length, number of annual trips, the setting(s) of their mobile or permanent clinics, the number and types of healthcare providers (Table 1).
Exploratory search
To determine current STMM activity, two authors (CH, GJ) independently conducted a hand search of the above STMM organisational websites. A data extraction form was used to document the date the website was last updated (“signs of life”), the date of the last known STMM trip and location, future trips planned and their proposed locations, additional qualitative information on substantive changes to mission scope, and current contact information. Disagreements were resolved by consensus between authors. This search was conducted between December 17, 2021, and March 17, 2022. If the website was inactive, a Google search was immediately performed to ascertain the continued online presence of the organisation at a different web address, using the organisation’s full name as the keyword.
Survey distribution and data collection
A SurveyMonkey online survey was created and distributed to the Medical Service Trip database using email addresses found either within the database itself or on the public website of the STMM and by using contact forms on the public websites. The survey was piloted among a convenience sample of three healthcare professionals and three laypeople to refine the questions, ensure comprehensibility and remove ambiguity. Pilot participants were timed on completion of the survey to ensure an average completion time of no longer than 5 minutes, a strategy implemented to maximise survey completion and minimise degeneration of response quality due to respondent fatigue. The final survey can be found in Online Supplementary Document, Appendix 1.
Each organisation was contacted by one of the authors with a standard email addressed to the listed primary contact between December 17 2021 and January 23 2022, using publicly accessible information on their organisational websites. The emailed introduction included the purpose of the study, its potential benefit to prospective volunteers and the literature, and a link to the results of a previously published study involving the Medical Service Trip database. No compensation was offered for the completion of the survey.
Two follow-up requests were sent to non-responders between January 23 2022, and March 16 2022, according to the Dillman approach to internet surveys, which maximises response rates through personalised, repeated contact.11 One final follow-up was sent through the organisational Facebook account, if available.
We attempted to contact all 359 organisations in the database and expected a survey response rate of 25–40% (n=91–145) based on previous similar studies using this database and typical response rates for external online surveys.12–14
Data analysis
Quantitative data from the survey were imported into Stata v.17 (StataCorp) for analysis. We began by examining descriptive statistics on organisational demographics and responses to each survey question. To mitigate potential concerns of non-response bias, we conducted Chi-square tests to assess whether demographic differences between groups (i.e., frequency and length of annual trips, mission and clinic type) resulted in differences in response patterns, with p-values of < 0.05 being considered significant. The Chi-square test is used to assess dependence between variables and is particularly useful if the sample size is small, the marginals are uneven, and certain cells have single-digit values.
For Question 8 (involving ranking factors leading organisations to cancel their STMMs), a weighted average was used to determine the importance to survey participants. Weights were applied in reverse (i.e., for 10 ranking options, the first choice had a weight of 10 and the last a weight of 1).
Score=(1w1+x2w2+x3w3…xnwn)total response countw=weight of the ranked positionx=response count for answer choice
Two investigators imported global comments and those specific to each survey question into Microsoft Excel for qualitative thematic analysis (GJ, CH). Each investigator read the qualitative responses to each question independently and developed a preliminary codebook used to assign descriptive codes to segments of the text. All authors reached a consensus on the definition of and use for each specific code, and a final codebook was created, which was used to re-code each response. The re-coded responses were then read to identify broader themes represented in the data.
RESULTS
Based on the results of the exploratory search, 22.5% (73/324) of previously active organisations had no website activity since 2020 or earlier, no longer existed, or had unclear website activity. Thirty-five educational STMM programs were excluded from the website analysis, as they had unclear entry requirements and unclear STMM-specific website activity. Ninety-six responses were received from the 87 organisations (Table 1) who responded to the survey (87/359, 24.2%). Nine of these responses were removed from the analysis, including eight identified as duplicates and one organisation that indicated that it had not operated an STMM in the last five years. Except for the type of clinic (p=0.042), the differences between responding and non-responding STMM organisations were not statistically significant. The response rate varied by question, but all questions had at least 81 responses. Of those responding on behalf of their STMM, 46/87 (53%) described themselves as executive members of their organisation and 44/87 (51%) as administrators. Twenty-five (29%) indicated that they were medical professionals, and 19/87 (22%) were previous overseas volunteers. Compared to organisations that did not submit a response, responding organisations tended to be more secular, more mobile, and more likely to run shorter trips.
The return to STMMs
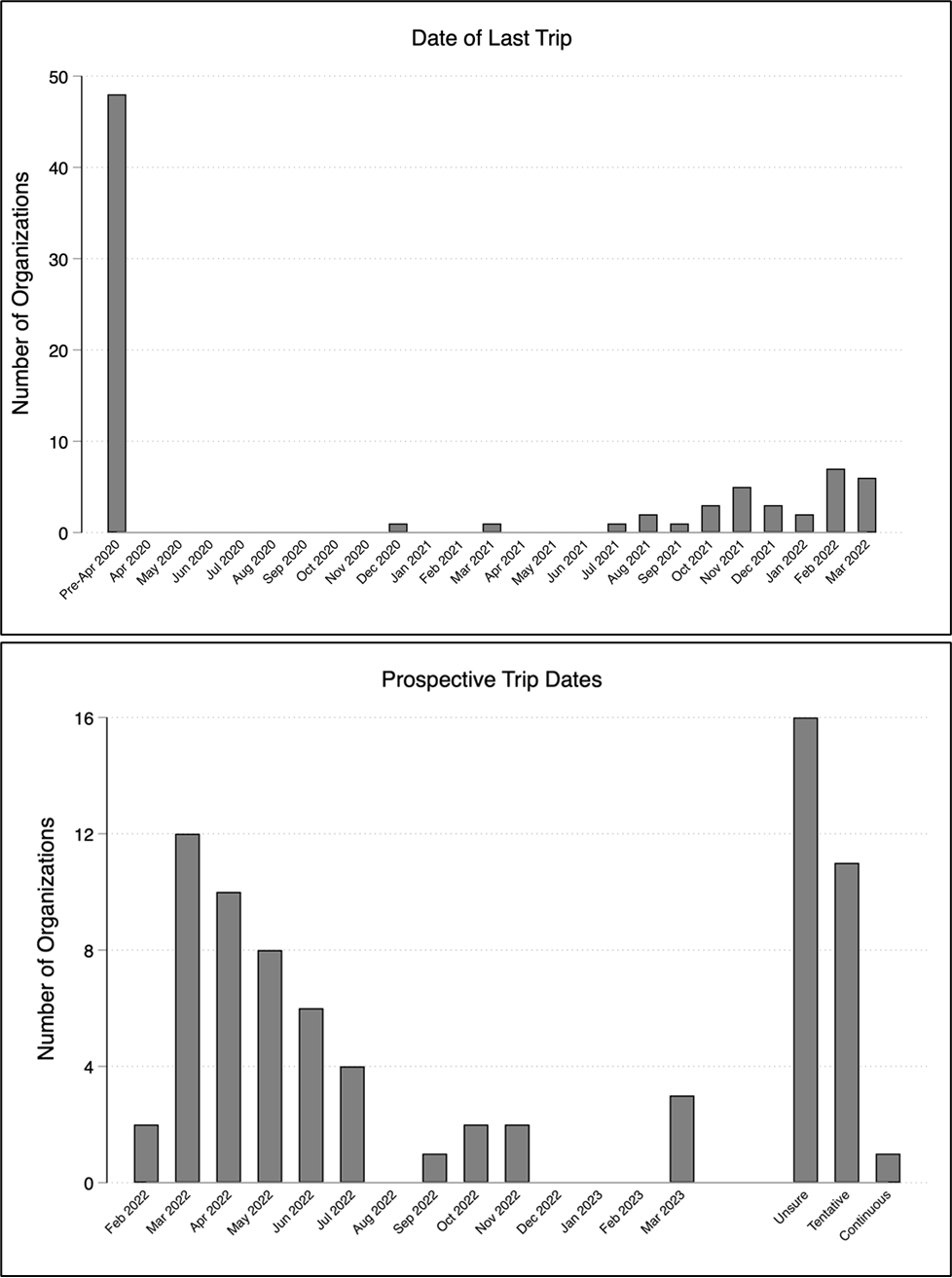
There was a bimodal split between organisations who reported having conducted their last STMM either prior to the declaration of the pandemic (48/80, 60%), and those who conducted one in the six months just prior to the distribution of the survey (26/80, 32.5%) (Figure 2). Ninety-six percent indicated that they would definitely (72/86, 84%) or probably (10/86, 12%) return to sending STMMs in the next five years, and most (46/83, 55%) intended to send an STMM within the next six months. Other organisations were unsure or only had tentative dates for their next trip (27/83, 33%). In the context of the pandemic, sixty-nine percent of organisations indicated that the number of volunteers they sent had decreased (21/84, 25%) or decreased greatly (37/84, 44%), mostly due to pandemic restrictions. However, a similar proportion (67%) of organisations anticipated the number of volunteers increasing (39/87, 45%) or increasing greatly (19/87, 22%) within the next five years.

Organisations perceived a more difficult funding environment than five years ago, with half of STMMs finding it somewhat (32/86, 37%) or much more difficult (11/86, 13%) to raise funds. Sixteen percent (14/86) found it somewhat easier, and 6% (5/86) found it much easier to raise funds. Most respondents were somewhat (38/86, 44%) or very (33/86, 38%) optimistic about the overall future of the STMM model, with one respondent mentioning their “partners request that we continue” and another confirming “in [their] experience, people are willing to go as soon as the pathways are open”.
However, five respondents expressed substantive concerns with the continuation of the STMM model. Their qualitative comments included the proposition that “there are a lot of significant issues related to medical missions”, that they “hope things change in the future”, that “the model should not be one-time service [without] follow up”, their belief that they “do not think the STMM model is appropriate any longer[,] except in the instances of disaster relief”, and that such trips “often contribute to colonialism, power dynamics, dependency and unsustainable interventions” while calling for “long-term health programs with infusions of volunteers focused on training, learning, and partnership” as an alternative.
Pandemic pivots
The majority of STMMs reported adapting their methods and objectives, with most STMMs changing slightly (26/87, 30%), substantially (34/87, 39%) or completely (12/87, 14%), and one organisation describing a move “to focus more on long-term sustainability and the ability of communities to sustain health initiatives even if outside groups cannot come in.” Only 15/87 (17%) reported that their methods and objectives had stayed the same. Respondents reported that their self-defined metrics for success had mostly remained the same (31/87, 36%) or changed slightly (33/87, 38%).
When asked to choose among new methods they had adopted for assisting host communities, 49% (42/86) of STMMs reported providing direct funding for local healthcare professionals, community healthcare workers and/or medical students. Fifty-eight percent (50/86) described sending additional equipment directly to host communities, with specific comments describing a focus on “humanitarian shipments versus organising brigades”. Twenty-nine percent (25/86) described focusing on training or teaching instead of direct care, including four organisations who commented specifically on collaborating more with local healthcare providers through partnerships, direct funding, additional “training for locally-based health guardians,” and efforts “to develop specialist training (residency, fellowship) in other countries.”
Regarding new technologies, 28% (24/86) of respondents reported adopting virtual care models, 14% (12/86) had moved to electronic medical records, and another 15% (13/86) reported adopting other forms of technological collaboration and innovation. Organisations specifically mentioned including “incorporating more [telemedicine] where able”, “conducting patient exams and follow-up care for patients with chronic conditions via telemedicine”, and that “physicians who are bilingual…are doing the patient encounters via Microsoft Teams. Our in-country partner schedules the visits and their nurses triage and present the patients to the US physicians.”
Barriers and challenges
Organisations were asked to rank the importance of specific barriers to the STMM model during the pandemic, with higher aggregate numbers indicating greater importance. COVID-19 restrictions at the country of origin (9.27) and destination (8.96) were closely followed by concerns about contributing to the spread of COVID-19 (8.83). These were followed by concerns over physical safety (8.24) and political instability (7.49) abroad and then by challenges in recruiting volunteers (7.45) and securing funding (6.84). The fulfilment of an a priori mission statement (5.31), unresolved ethical concerns regarding the STMM model (4.30), and hosts identifying no further need for volunteers (3.42) were ranked lower by respondents.
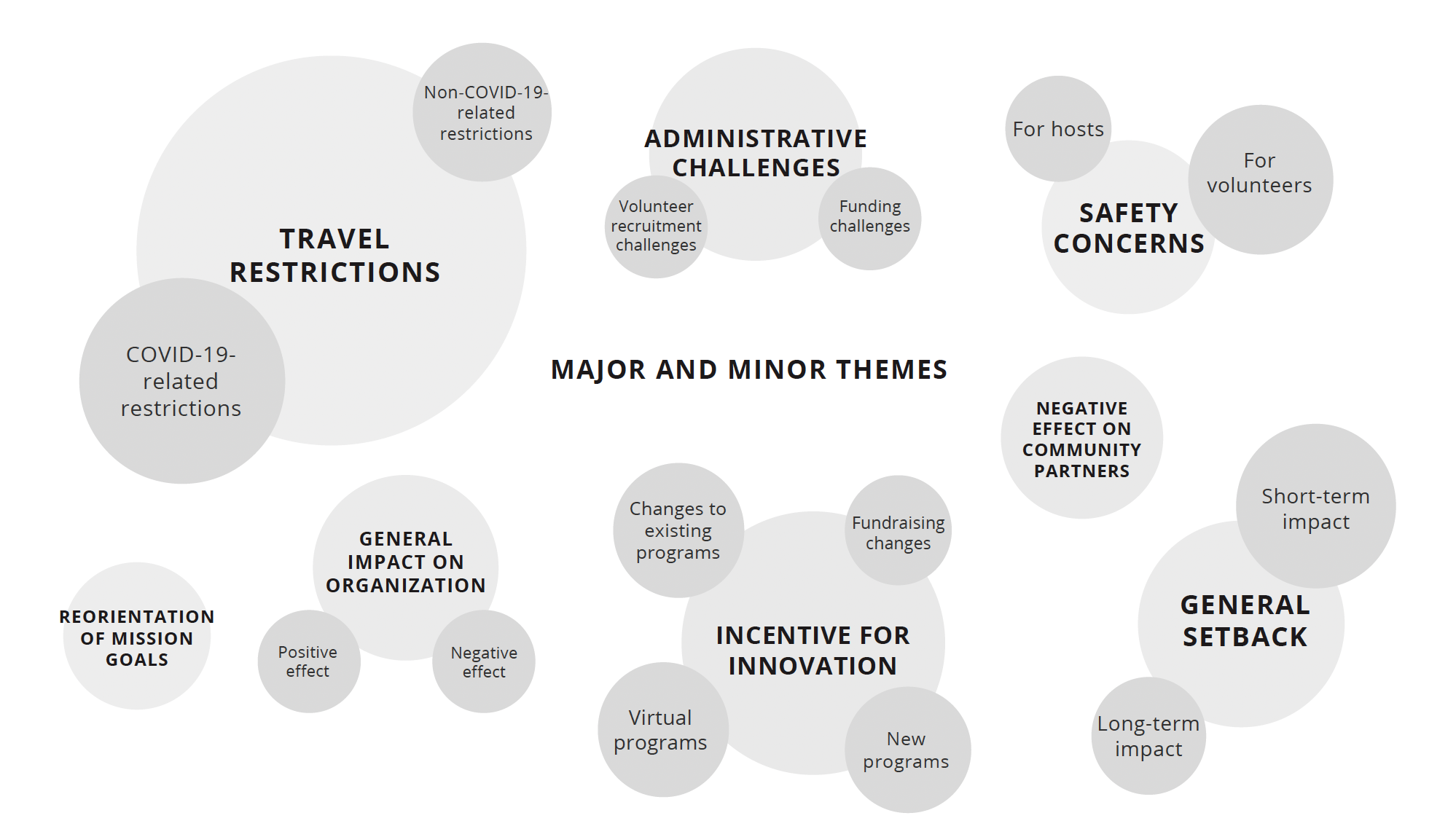
Respondents submitted a total of 90 qualitative comments regarding the general effect of the pandemic on STMM projects. Thematic analysis of the perceived effect of the pandemic on STMMs (Figure 3) revealed certain major and minor themes among the responses. These included the inability to deploy STMMs (48), the pandemic as a catalyst for innovation (20), the challenge of decreased volunteers and funding (19), the generally negative effects on organisations (23) and community partners (6), the need to reimagine STMM mission parameters (13), safety concerns for volunteers (3) and hosts (3), and the pandemic as a short-term (14) or long-term (2) setback.

DISCUSSION
The COVID-19 pandemic substantially reduced the activity and funding of STMMs in LAC and forced organisations to consider alternative models of humanitarian engagement with host communities abroad. To our knowledge, this is the first study to explore STMM organisations’ perceptions regarding the pandemic effects and the strategies they used to address these unprecedented challenges. Given that no formal system exists to integrate and track STMMs on a grand scale,15 this study also represents the first longitudinal analysis of the turnover of the STMM landscape over the last seven years.
We found unexpected resilience and optimism among the humanitarian organisations who responded to our survey, with most organisations intending to return to business as usual over the next two years. However, our findings certainly reflect a selection bias that accords greater weight to those organisations most likely to be active in the future. This study also represents perceptions and outlook at a specific point in time, given that our data collection took place during a broad period of reopening from the pandemic lockdowns which had previously been applied both in North America and across LAC.16
Before the pandemic, numerous academic sources in the global health community had advocated for increased attention to ethics, sustainability, and community partnerships in the STMM space.17,18 The move towards virtual and alternative forms of medical aid indicated by our results may suggest that the pandemic intensified the growing push towards host-community-driven healthcare solutions and coincides with an increased recognition that routine primary medical care is better provided by in-country medical staff than by foreign volunteers. Anecdotal evidence in the literature aligns with our general findings. Others have observed that STMM organisations have adapted to circumstances by supporting more in-country staff, purchasing equipment, paying directly to treat sick patients with antibiotics or surgery, and training local health workers via e-learning or zoom.19
Strengths and limitations
The strengths of this study include using a broad sample of STMMs that have been active across LAC using a comprehensive database of such trips. Furthermore, the high response and completion rate was in excess of typical anonymous surveys,13,14 which suggests high motivation and engagement among respondents. We used a combination of quantitative and qualitative assessments to allow for an open-ended review of STMM perceptions regarding the effects of the pandemic. A supplementary online search also allowed for an overview of the evolution of the STMM landscape and to assess the status of organisations that did not respond to the survey.
As discussed above, one important limitation of this type of study is response bias, given that those organisations that respond to an online survey may be fundamentally different from those that do not, although we have attempted to address this through a comparison of the features of responders versus non-responders. Second, the reliability of the survey responses is also contingent upon the reliability of the specific organisational representatives since only the primary contact for each organisation was solicited to complete the survey on behalf of their organisation. Finally, it should be noted that while the original database represents the most comprehensive attempt to gather information on the breadth of STMM activity in LAC to date,8 its accuracy depends upon the online presence and public profile of such organisations and is, therefore, ultimately a convenience sample.
CONCLUSIONS
The unprecedented challenge of the COVID-19 pandemic and its resulting public health restrictions brought many STMMs to a halt and strained sources of funding and volunteers, leaving many organisations still uncertain of when they will resume their projects. Despite these challenges, many STMMs organisations have shown resilience and capacity for innovation, often adapting their aid model to prioritise the distribution of food, personal protective equipment and offering virtual trips.
Future studies should address the long-term impact of the pandemic on models of virtual and in-person STMM care in international settings. Further qualitative and quantitative studies should address the effect of the pandemic on access to healthcare and health outcomes of host communities, as well as overall stakeholder satisfaction with the alternative aid models being proposed and implemented in partnership with humanitarian organisations.
Ethics approval
All study protocols were approved by the Tri-hospital Research Ethics Board (THREB) in Ontario, Canada.
Data sharing and availability
The data underlying this article will be shared on reasonable request addressed to the corresponding author.
Funding
None.
Authors’ contributions
CD conceived the study and designed the study protocol; GJ and CH conducted data collection and analysis. All authors were involved in drafting the manuscript. All authors read and approved the final manuscript. CD is guarantor of the paper.
Competing interests
None declared.
Correspondence to:
Christopher Dainton, MD, CCFP(EM)
835 King St. West, Kitchener, ON, Canada.
[email protected]