

Infant immunization is an effective strategy for reducing infectious disease morbidity and mortality. Since the 1990s, annual infant mortality from vaccine-preventable infectious diseases has decreased from 14 million to five million due to worldwide efforts by national policymakers to enforce recommended vaccination schedules.1 In 2016, vaccine coverage across 152 high-burden countries for the first dose of Diphtheria Tetanus Toxoid and Pertussis (DTP) and measles-containing vaccine were 94% and 93%, respectively. Coverage falls short, however, for widely implemented birth-dose (BD) vaccinations—Bacillus Calmette-Guerin (BCG) and the first oral polio dose (OPV0)—with BCG coverage at only 37% in the same 152 countries.2 While national policies have improved vaccine coverage, the next step is addressing the unique challenges of timely BD vaccine delivery.
The hepatitis B vaccine is the first cancer-preventing vaccine,3 and is included in routine child immunization schedules globally—since the 1980s in high-income countries and 1997 in sub-Saharan Africa (SSA). The World Health Organization (WHO) recommended including the hepatitis B birth dose vaccine (HepB-BD) in national guidelines in 2009. Historically, infants received the first dose of the vaccine at six weeks, which is too late to interrupt mother-to-child transmission (MTCT). If administered within 24 hours of delivery and followed by two or three additional doses, HepB-BD is >95% effective in preventing MTCT.4–6 Countries like the Democratic Republic of the Congo (DRC) are moving to include HepB-BD in their national immunization schedule.3 However, without a clear implementation strategy, delivery of an additional BD only adds to the complexity of timely delivery.7 Therefore, as countries streamline universal HepB-BD with existing BD vaccines, it is critical to explore the existing unique determinants to delivering timely BD vaccines.
To our knowledge, no qualitative studies have reported on determinants of BD vaccine uptake in a low-resource setting. This study aims to support decision-makers by identifying barriers and facilitators of timely BD vaccine delivery in Kinshasa Province, DRC, through interviews with individuals across the vaccine care continuum.
METHODS
Study design, setting, and patient population
We conducted semi-structured qualitative interviews in seven health facilities across Kinshasa Province, DRC. We purposefully sampled health facilities with maternity and vaccine wards. We chose the five most prominent facility types in the province—private, public, Catholic, Protestant, not-for-profit (NFP)—and selected a sample of seven facilities (Figure 1). Kinshasa Province is predominately urban, so we selected facilities accordingly - six urban and one rural of 983 facilities in the province.8 Since Catholicism is the primary religion in the DRC, which represents a significant provider of health services, we selected two Catholic facilities. The facilities ranged in size and therefore experienced a range in volume of monthly deliveries from 40 to 300. Vaccines in DRC flow from external donors—the Vaccine Alliance (Gavi), the United National Children’s Fund (UNICEF), and the WHO—to the National Immunization Program (PEV) and the health zones, and finally to health facilities where vaccines reach the consumer—the mother-infant pair (Figure 2).9,10 We invited a sample of up to two expectant mothers and three facility informants to participate from each facility, in addition to vaccine officials at the health zone and national levels. Eligibility requirements included: age ≥18 years and understanding of either French or Lingala, the two local languages in Kinshasa.


Data collection
Interviews were conducted using two semi-structured interview guides with open-ended questions, available in French and Lingala. The interview guides were developed using existing relevant literature11–15 and reviewed and validated by the entire study team. To understand administrative barriers to HepB-BD, we interviewed decision-makers and/or providers (hereafter ‘informants’) from various levels of the health care continuum, including midwives, immunization staff, heads of maternity and immunizations, and vaccine officials at the health zone and PEV. We interviewed primigravid (8) and multigravida (6) mothers to elicit perceptions about infant vaccination from new and experienced expectant mothers. The interviews were led by a bilingual (French/English) PhD candidate (AB) with education and experience interviewing study populations. Interviews were live translated from Lingala to French by a bilingual (French/Lingala) study team member (PN) with a medical doctorate and many years of experience interviewing study populations.
Staff working the day of the facility visit and mothers presenting for routine antenatal care (ANC) were approached for enrollment. Interviews were conducted in-person, in private rooms, in French or in Lingala with simultaneous French translation, and on the same day as study enrollment. Interviews were audio-recorded and lasted 15-60 minutes.
Data analysis and framework
The audio-recorded interviews were transcribed and translated to English by a bilingual study member (AB); transcripts were then imported to MAXQDA2020 for coding and analysis. Deductive codes were generated using existing literature on vaccine uptake and administration barriers. Themes were established and harmonized through iterative analysis. AB coded and analyzed data alongside CEM. AB and CEM reviewed the transcripts for patterns and major sources of saturation to organize the findings into major themes as they were received. Theme saturation was reached when codes or categories described a similar phenomenon on repeated occasions across multiple respondents.16 AB and CEM met regularly and compared and contrasted similarities and differences among the coded interviews. Finally, the study team reached consensus about what patterns of codes constituted a theme and the prevalence of the pattern required for saturation.
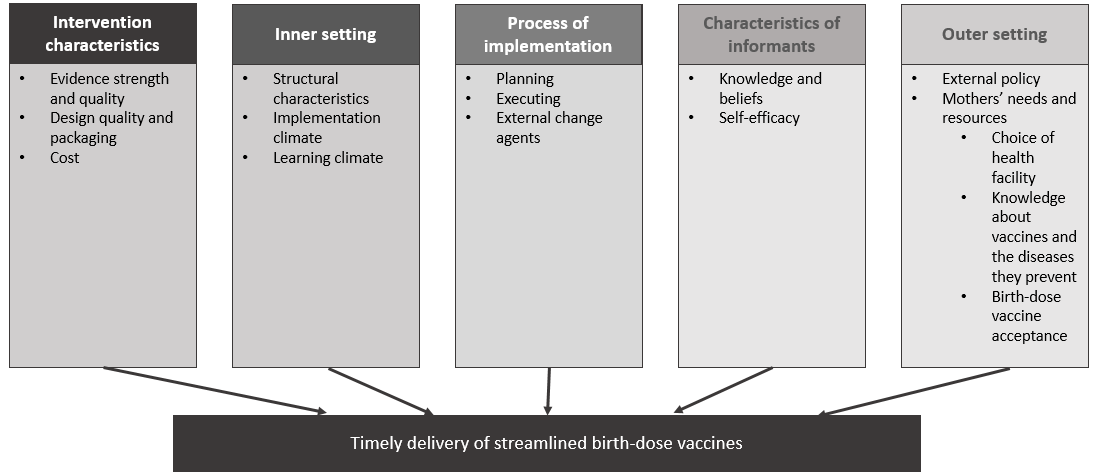
The data analysis was guided by the Consolidated Framework for Implementation Research (CFIR). The CFIR organizes key barriers and facilitators into five domains—intervention characteristics, inner setting, outer setting, staff characteristics, and the implementation process—of 37 measurable constructs.17 Use of the CFIR framework allowed the study team to account for contextual factors.
Ethical considerations
Informants and expectant mothers provided written, informed consent. All consented to the audio recording of interviews. Data were de-identified prior to analysis and were stored on a secure server with copies of the recordings. Institutional Review Boards at UNC-Chapel Hill and the Kinshasa School of Public Health approved the study protocol [UNC IRB 21-0014; KSPH IRB 0001 1-04101-00001365292-20].
FINDINGS
We approached 32 participants (17 informants and 15 expectant mothers) and conducted semi-structured interviews with 30 participants (16 informants and 14 expectant mothers) in June-July 2021 (Table 1). One informant declined due to medical reasons, and one mother declined due to wait time. Interviewees were recruited from seven health facilities, two health zones, and PEV. Our analysis identified 13 constructs related to the success of timely and streamlined vaccines (Figure 3). We organized the sections by CFIR domains (Table 2) and include additional quotes corresponding to the domains (Online Supplementary Document).

Intervention characteristics
Evidence strength and quality
Many informants spoke to the effectiveness of the two existing BD vaccines, BCG and OPV0. In addition, many informants were aware of trials to pilot the HepB-BD vaccine in the DRC, such as a HepB-BD feasibility study conducted in Kinshasa-based maternity centers.18 Further, a few informants mentioned inclusion of HepB-BD in WHO recommendations.3
Design quality and packaging
A critical barrier to BD vaccinations raised by informants was the design quality and packaging of BCG vaccine. In the DRC, BCG is only available in 20-dose vials, and opened vials have a six-hour shelf life. National policy states that a vial should be opened only when 10-20 newborns are present. In the words of one informant:
“Yes…with the strategy, we need at least 20 newborns to open a vial, that’s why we ask that they come back on Wednesdays. We have records of all of the newborns born. We call them every Wednesday and tell them to come back to the health facility as not to give it to them too long after birth” Informant NFP 3.
Further, a PEV informant described vaccine wastage as a provider-level performance gauge set by district-level health zones:
“Beyond their day-to-day work, [the providers] have their performance metrics to consider and they don’t want to inflate their rate of vaccine loss” Informant PEV 1.
Cost
Informants reported that mothers must buy a vaccine card to track infant immunizations. The card price varied between facilities from 1 USD in a rural facility to 15 USD in a private facility. All primigravid mothers reported not knowing about a fee for the vaccine card prior to delivery. For example:
“They will give us a card after we deliver…for the payment, they haven’t told us anything” Mother NFP 2.
All facilities but one reported transferring multiple complicated births to other facilities each month. Those mothers would pay for a vaccine card and begin infant vaccination at the facility where they delivered, and often returned to their preferred facility to continue infant vaccine visits. When asked whether the health facility would accept vaccine cards from other facilities, every informant except for one at a public health facility responded to the contrary:
“No, if she begins her infant’s vaccine care elsewhere, and decides to come here to continue it, she must repurchase a card here [but vaccines will not be repeated].” Informant Catholic 4.
Inner setting
Structural characteristics
Informants reported acquisition of vaccines in two ways: 1) daily retrieval by facility staff from vaccine storage at a health zone, and 2) storage at individual facilities in a solar fridge, provided through a selection process controlled by PEV and external donors. Facilities in the latter group may store monthly vaccine allotments for themselves and nearby facilities.
Four facility informants mentioned electricity outages posing a significant barrier to efficient vaccine storage; for example:
“Now, vaccines are products that must be conserved in very specific conditions so that the antigen is active. If the required conditions are not reached, we stand the risk of providing placebo vaccines. So, even us here who have electricity, we realize that we stand the risk of experiencing electricity outages. These outages can alter the temperature at which the vaccines are kept” Informant Public 3.
A solution suggested by three informants was regular supervision of the cold-chain temperature to ensure vaccine viability:
“Every morning I am obligated to travel and verify the temperature at which the vaccines are being stored and to record it, and to make sure that the health workers in the facility are doing this” Informant Health Zone 1.
A barrier to timely BD vaccination is that vaccines are stored in fridges near the vaccination ward of the facility, separate from the delivery/newborn wards. Six informants at the facility level reported a smaller fridge where vaccines may be kept near the delivery ward, but only three reported storing BD vaccines in these fridges. Informants reported a significant physical distance between the delivery and vaccination wards:
“And for fridges… the maternity does not vaccinate, it is the vaccination nurse that oversees the number of children available for the vaccination…. the vaccines are kept in the fridge and the nurses are in charge of vaccinating” Informant Protestant 1.
Implementation climate
Mothers and informants expressed optimism for innovative vaccination techniques. Several informants shared exciting new approaches to increase vaccination rates and decrease loss-to-follow up, such as community health worker (CHW)19 outreach programs, mHealth solutions, malaria prevention incentives, and the expansion of rural health posts:
“Every time now that a mother comes in to have their child vaccinated, we register the moms, we collect their telephone number and their address, so every time they have an appointment coming up, they will receive a text message reminder of their appointment. This way, you will not be distracted and remember your date. Since we started this study, I would estimate though that we have decreased the loss to follow-up rate, from 21% to 16-18%” Informant Public 3.
Learning climate
Some informants expressed a need for procedural training of staff across disciplines. Often midwives who care for infants in the first days of life do not receive guidance about vaccine administration. An informant suggested:
“When we organize trainings or briefings about vaccination, we target vaccine providers from health facilities. We do not often see the midwives, even though they are the door for infants to enter into the [vaccine] system. So, it is really important to provide them too with briefings or trainings” Informant PEV 1.
Process of implementation
Planning
Many informants mentioned national immunization guidelines directing decision-making processes, but some provided inconsistent reports on several key aspects. For example, many informants referred to national immunization guidelines directing immunization policy, but some incorrectly interpreted these guidelines. When discussing BCG vials, one informant stated:
“We are not obliged to vaccinate infants unless there are 15 of them. If 3 or 5 are born, then we do not vaccinate them” Informant Catholic 1.
While another stated:
“The ideal is 20. But they have authorized us to provide the vaccine when there are 10 infants. So, when we have 10 infants, we administer 10 and lose the other 10” Informant Private 1.
Evidently, guidelines on BD vaccine administration varied across accounts from providers.
Executing
A common barrier expressed by all informants and many mothers was the stockout of medicines, especially BCG vaccines, hindering timely vaccine uptake. One mother stated:
“There’s a problem with the BCG. There aren’t enough vaccines. Women who deliver here sometimes have to wait one month [for their infant] to receive the vaccine” Mother Private 2.
Informants described a nationwide stockout of BCG from May-July 2021. Stockouts were reported to be unpredictable, and facilities did not have adequate supplies.
External change agents
A few informants mentioned donors such as Gavi and UNICEF as providers of vaccines and solar fridges to overcome storage and quality constraints at the facility level. For example, the health zone informant said:
“UNICEF provided us with nine refrigerators—seven fridges in the facilities and two here in the health zone. They provided the new fridges in March” Informant Health Zone 1.
Characteristics of informants
Knowledge and beliefs about the intervention
Strong informant support for timely BCG and OPV0 vaccines was due to respect for PEV BD mandates. Many informants would welcome HepB-BD if research and policymakers supported it:
“They told us that we should introduce that [HepB-BD] at birth. And we await the period that we begin introducing it. Because we were well informed by PEV that there will be an introduction but until today, nothing” Informant Health Zone 2.
Self-efficacy
During ANC visits, midwives reported focused more on maternal care than on infant vaccination. As a result, provider willingness to communicate with mothers about BD vaccines was low. Most providers expressed vaccine knowledge and confirmed dissemination to mothers during ANC visits, but none of the mothers supported these claims. Mothers only reported education about receiving tetanus vaccine themselves during pregnancy. One mother stated:
“What is important is to help us understand. During the visits, [the midwives] need to go into more detail because here we are in the dark [about vaccines/diseases]” Mother Catholic 1.
Outer setting
External policy
All informants were aware of national guidelines to provide BCG and OPV0 at birth. All facility-level informants also stated willingness to accept inclusion of HepB-BD in the immunization schedule if PEV mandated it.
Mothers’ needs & resources
Choice of health facility
Vaccine cost and availability played a minimal role in mothers’ choice of facility. Many, even experienced, mothers did not know the cost of vaccine care and only vaguely knew which facilities offered vaccines. Instead, mothers revealed that their choice of a health facility was based on three factors: quality of care provided, distance to the facility, and recommendations from their family/community:
“[Seeking care at this facility] was my mom’s advice. My mom delivered here, and my big sister delivered here too. My mom told me that there is good care for the sick and a good quality of health here” Mother Catholic 4.
Mothers mentioned distance to a delivery facility influencing their decision in two ways. They either chose the closest and most convenient facility, or a farther away but ‘higher quality’ facility (and may continue infant immunizations at a closer facility).
Many informants agreed with the first two motives—the quality of the facility and distance— in mothers’ choice of facility. One informant cited another factor associated with facility choice: affiliation with a community and/or religion.
“What motivates here is distance, that is an aspect but not the only aspect. The second aspect is partnership. Say the partnership to a community, or perhaps to a religion. You will see that a Catholic would like to visit a Catholic facility. The third is the perception by the community of the quality of service by the health facility… a woman would say that she wants to go in this facility because it is clean, because it is presentable, it is a bit of that” Informant PEV 1.
Knowledge about vaccines and diseases they prevent
Only five of 16 expectant mothers stated having knowledge of HBV. Mothers who indicated having knowledge about HBV understood it only as a disease and were unfamiliar with prevention measures. Further, one mother believed it to be a disease that mainly afflicts infants:
“I don’t know much [about HBV], but I’ve heard it talked about. It is more the children who suffer” Mother NFP 1.
Similarly, mothers generally knew little about infant vaccines. Most primigravid and multigravida mothers could not provide details about any vaccines received during infants’ routine vaccine visits. Experienced mothers could name BCG or demonstrate where infants received the vaccines on the body but could not explain which diseases were prevented by specific vaccines:
“Kids receive vaccines. I don’t know the names of the vaccines, but one is given orally and the other in the arm” Mother Public 2.
When provided the chance to ask questions during the interview, many mothers asked for more information about HBV, the risk it poses to their babies, and prevention methods, suggesting openness to vaccine education:
“I want to know what hepatitis B is and more about the vaccines” Mother Protestant 1.
Birth-dose vaccine acceptance
Every mother expressed comfort with the current immunization schedule, and vaccinating their newborns within 24 hours of delivery. None of the mothers reported hesitancy about vaccines for their infants. When prompted, a mother responded:
“Yes, I would be very comfortable with [my child receiving a BD vaccine] because this vaccine will give my child force and strength. If there is a disease that attacks my child, they will be protected” Mother Public 2.
While the mothers did not express vaccine hesitancy themselves, seven mothers reported other family or community members expressing hesitancy:
“My maternal aunt refused vaccines for her kids. She thought that vaccines are bad for kids” Mother Catholic 4.
In addition, while the primary focus of our exploration was to understand facility-level vaccine hesitancy, a comment by a health zone-level informant in relation to community uptake of vaccines offered during mass vaccine campaigns was a striking indicator of community level vaccine hesitancy that mothers inevitably experience:
“Vaccines remain until now the best method for prevention. But the quality suffers because there are too many speculations, it is perhaps you—the whites—who are putting confusion into the heads of the blacks.” Informant, Health Zone 2.
The informant believed that fake information and media arriving from exogenous sources are a serious risk to vaccine uptake across the DRC. He stated that this was evident by the consistent decrease in vaccine uptake during annual mass campaigns in the last few years.
DISCUSSION
This study is one of the first to identify determinants of HepB-BD vaccine uptake reported through interviews with informants and expectant mothers. Applying the CFIR domains, we found significant barriers to timely BD vaccines in Kinshasa, DRC, including the multi-dose vaccine vials which determined when facility staff could vaccinate newborns; logistical concerns with regular national vaccine stockouts and, where available, inability to store vaccine in some instances; complex and unsynchronized vaccine fees across facilities; inadequate communication across delivery and vaccination wards; and limited and at times incorrect understanding of vaccines among mothers and other community members.
Many informants and mothers expressed a desire for change, progress, and learning, but within a top-down system in DRC, dissemination of HepB-BD and streamlining guidelines must begin at the national level. A study of five SSA countries that introduced HepB-BD found the weakness of national policies and lack of written guidelines to deliver timely HepB-BD a significant barrier.20 Informants confirmed their willingness to adapt BD vaccine initiatives, if supported by research and policy makers. We recommend harnessing that enthusiasm by developing clear guidelines for HepB-BD implementation at each level and conducting multiple trainings across the healthcare delivery spectrum, beginning at the level of national decision-makers and external funders and continuing to midwives and staff who would administer vaccines.
Packaging of BCG vials has implications for streamlining BD vaccines. The DRC receives support from Gavi, which requests that countries reduce their wastage to 15% (3 doses) for every 20-dose BCG vial.21 It is therefore standard across SSA facilities to conduct daily to monthly batching of doses, depending on the volume of births in the facility.22 The low volume of deliveries at rural or smaller facilities poses a critical barrier to BCG vaccination. Like HBV, BCG is ideally administered within the 24-hour window following delivery, with reductions of neonatal mortality by more than 40% compared to outside the 24-hour window.23,24 The balance between reducing wastage and increasing essential coverage is a barrier to BCG coverage.22,25,26 A solution to reducing wastage is to make lower dosage vials available. In Zambia, facilities using 5-dose vials had 47% lower waste than those using 10-dose vials.22 While HepB-BD is typically offered in a 10-dose vial, HepB-BD lasts up to one month after the vial is opened (unlike BCG, which only lasts 6 hours).3 However, if facilities hope to streamline the delivery of all BD vaccines and discontinue the newborn-batching approach, the size of BCG vials must be revisited.
Storage across and within facilities was a significant barrier within the inner setting domain. If a facility did not have capacity to store vaccines, staff traveled daily to collect vaccines. In addition, the limited availability of other resources, such as fuel and vehicles, was a common barrier to collecting off-site vaccines. When facilities had vaccines on-site, cold chain temperature surveillance posed a threat to the effectiveness of the BD vaccines.7 In addition, some informants reported only storing BD vaccines in the primary fridge, and not near the delivery ward. Midwives reported not having access to the fridge and needing to coordinate vaccine administration with vaccine staff. These administrative barriers can cause further delays in the timeliness of the BD vaccines. The WHO recommends storing HepB-BD in the delivery ward to facilitate timely vaccination, especially if the storage ward requires special access permission—which was often the case in the study facilities.3 We recommend clear guidance for facilities in line with these recommendations on the adequate storage of vaccines.
Gavi and national-level co-financing cover the cost of infant vaccinations and staff administration fees in DRC.27 Despite this financing, mothers have to pay prohibitive fees for services.28 To improve vaccine access, WHO recommends that HepB-BD (and other vaccines) be supplied to facilities at no cost and that facilities should not charge families for vaccine administration.3 Therefore, we recommend national policy mandating free vaccine services for mothers. At the same time, national programs and their partners should appropriately compensate health facilities for their efforts.
We endorse training facility staff (midwives and vaccine staff) and education for mothers about BD vaccines. Informants reported providing thorough education to mothers during ANC visits, though most mothers could not name infant vaccines. We recommend more explicit guidance and educational material to facilitate vaccine communication pre-delivery. The provision of communication tool-based training for health workers has been shown to have a positive impact on vaccine uptake.29,30 Options may include employing audio-visual educational materials,31 or utilizing social workers instead of midwives to present visual aid tools to parents.32 Improving mothers’ knowledge will help combat vaccine hesitancy and increase mothers’ understanding of the benefits of timely and complete vaccination. Midwives should also receive training on vaccine delivery to streamline BD administration.
The outer setting factors of CFIR, such as mothers’ socio-demographic factors, attitudes, and knowledge about vaccines on health-seeking behavior, are essential when considering BD vaccines. These factors influence the final link in the vaccine distribution process, consumer uptake. The literature suggests that the strongest predictor of not receiving timely BD vaccines is the cost of vaccines,28 and we thus expected vaccine fees to influence a mother’s health-seeking behavior. However, we found that mothers knew little about cost and availability, and instead based decisions about which facilities to attend on the facility’s quality of care, distance from home, and recommendations by family and friends. In addition, contrary to national evidence suggesting a rise in vaccine hesitancy,33 our findings indicated that mothers were very comfortable vaccinating their newborns. One facility informant suggested that vaccine hesitancy is not a problem upon initial delivery, but that hesitancy is fostered once the mother-infant pair leaves the facility and is influenced by community-level hesitancy. Increasing maternal health literacy can combat vaccine hesitancy at the individual and community levels to increase vaccine coverage.34 Sensitization campaigns through social media, mass media, or CHWs should target not only mothers, but also community members.29
Limitations
Our study has a few limitations to note. First, as a typically sized qualitative study, a sample of 16 informants and 14 expectant mothers within a large urban area may not capture all viewpoints. We iteratively reviewed transcripts to ensure that we reached thematic saturation, which is a more valuable measure than sample size in the realm of qualitative research. Secondly, we recruited all mothers from ANC visits, and therefore the participants are predisposed to maternal and child healthcare—which includes immunization care—compared to mothers who deliver at home or who do not seek antenatal care. As homebirths are no longer legal in the DRC and an estimated 80% of births occur in facilities, this sample aligns with future HepB-BD implementation. Third, all participants were recruited in a predominately urban setting, and therefore the findings may be less generalizable to rural settings. Finally, some phrasing may have been lost in translation due to multiple languages; this was countered by the expertise of natively bilingual investigators who administered, interpreted, and analyzed the interviews.
CONCLUSIONS
Using the CFIR framework, this study integrates perspectives from facility informants and expectant mothers to inform future national policy and implementation of the HepB-BD in DRC. These stakeholder-driven findings should guide the streamlining of timely BD vaccinations upon HepB-BD implementation.
Acknowledgments
We thank all of the women and informants who participated in this study. We also thank the staff at the maternity clinics, and provincial and national health authorities. Ethical approval for this study was received from the Institutional Review Boards at UNC-Chapel Hill and the Kinshasa School of Public Health approved the study protocol [UNC IRB 21-0014; KSPH IRB 0001 1-04101-00001365292-20].
Funding
AB reports a grant by the Drusilla L. Scott Summer Research Fellowship. CEM reports funding from the UNC Graduate School, UNC School of Medicine Office of Global Health Education, and the Infectious Disease Society of America. PT is funded by grants from the NIH (K08AI148607) and from Novavax, Pfizer and Merck, outside of this work. PT also reports research support from a fellowship through the American Society of Tropical Medicine and Hygiene–Burroughs Wellcome Fund and from Gilead Sciences, Inc, outside the submitted work. PT and MY report non-financial support from Abbott Laboratories. MY also reports funding from NIH (R01HD087993, R01HD105526, U54CA254568, U01 AI096299).
Authorship contributions
AB, PT, BF, CMS, and MY designed the study. AB, PN, CEM, NM, KM, and PB contributed to the field work and interviews. AB, CEM and PT coded the interviews. AB wrote the first draft, with contributions from PT, BF, CMS, MY, CEM, NM, KM, and PB. All authors edited and revised the final manuscript and approved the final version.
Competing interests
The authors completed the Unified Competing Interest form at http://www.icmje.org/disclosure-of-interest/ and declare no conflicts of interest.
Correspondence to:
Alix Boisson, Department of Health Policy and Management, Gillings School of Global Public Health, The University of North Carolina, Chapel Hill, North Carolina, USA.