










In its 2017 Comprehensive Food Security and Vulnerability Analysis, the World Food Programme (WFP) found that, at any given time, around 16% of Cameroonian households were food insecure (3.9 million people); of these, 1% were severely food insecure (around 211,000 people).1 Various factors impairing food security in Cameroon have been investigated during and after the 1990s economic crisis,2 when, along with an increase in under-5-mortality, the prevalence of childhood stunting accompanied by underweight has increased from 23% to 57.7% (1991-2011). According to its purpose to reduce food insecurity, within the Consumer Products Supply Regulation Mission (MIRAP) in 2009, the Cameroonian government put in place travelling food markets to sell food at rates aiming to bring down food prices in local markets.3 The strategy of reducing food prices did not effectively work, as it did not consider the low purchasing power of families and, in particular, of women in charge of defining the daily meals.4 Indeed, apart from the purchasing power,3 a complex relationship exists between culture, food availability, infant feeding practices and maternal nutrition.5 In Cameroon, stunting goes beyond the poverty line as 12% of children in the wealthiest quintile are stunted, suggesting that this is not only a food access issue6 but an inadequate nutrition competence. Appropriate knowledge of children’s nutritional needs and feeding practices are therefore required.4 Feeding is both a biological and cultural phenomenon.5 Specific food categories (viper meat, palm wine, colostrum and eggs) are attributed to physical and social characteristics and are either (dis)qualified for children and their mothers.7 Food taboos contribute to protein-energy malnutrition common among infants and children in poor socioeconomic groups. Food security would benefit from health literacy in terms, e.g., of reduction of waste of fresh fruits and vegetables that are generally available and affordable but poorly consumed.8 As shown by research findings from Nigeria, many nursing mothers utilise local food ingredients to formulate weaning foods for their babies. While the nutritional composition of these foods is expected to be high in quality, they are also suitable as weaning foods, particularly for infants from low socioeconomic level families who do not have access to commercial weaning foods.9 This calls both for advocacy favouring caregivers and children nutrition education, focusing on a healthy food selection with culture bears in mind. Indeed, social networks do influence infant and child mortality,10 and communities contribute prominently.11 With the recent school schedule made by the Ministry of Basic Education, the preschool and primary school children spend 8 hours (7:30 am-2:30 pm) in school. Most children skip breakfast and depend on either their packed lunch or meals from school vendors or the school canteen. Dietary and eating habits are formed during childhood.12 To prevent unhealthy diet and eating, individuals should acquire appropriate habits in childhood. Few studies have been published on the impact of nutrition education in primary schools in sub-Sahara Africa,13 and limited work has been conducted on feeding practices of children in Cameroon.14,15 Civil societies and private organisations, even public bodies, implemented only a few nutrition education programmes in Cameroon, with limited coverage. Outputs of these initiatives are in current law and regulations but are out of date, non-comprehensive and incomplete; their enforcement at date cannot be effective. Nutrition education is not taught as a subject in schools; it is barely introduced as a side subject. A study developed at the Confidence Primary School of Makèpè, Missokè, Douala, Cameroon, underlined poor knowledge of feeding practices among children (6-14 years old).15
Nutrition education is any combination of educational strategies accompanied by environmental support designed to facilitate voluntary adoption of food choices and other food- and nutrition-related behaviors conducive to health and well-being. Nutrition education is more likely to be effective when it focuses on behaviour and action rather than only knowledge and is linked to educational theory.16 In this regard, exposure to toxic (natural and man-made) chemicals has emerged as a shared aspect in fighting all forms of malnutrition, especially in chronic malnutrition.17 Weaning foods prepared under unhygienic conditions are frequently heavily contaminated (e.g. aflatoxins) and cause diarrheal diseases and associated malnutrition.18–20 With poor preparation, preservation and hygiene practices, many cases of food poisoning occur in Cameroon.21 Toxic exposures may worsen the micronutrient status e.g. by increasing the nutritional requirements; vice versa, imbalanced diets and micronutrients deficiencies may increase the vulnerability to the effects of toxic substances and alter body defence systems.17 Besides advancements in African and international knowledge on nutrition, food safety and their interactions,22 the translation of scientific research and knowhow into awareness of consumers (children), citizens (parents/caregivers), school canteen operators, and school administrators remains particularly poor. Contaminated foods and poor hygiene practices caused 1.5 billion diarrhoea and upper respiratory tract diseases in children each year. Hands are a key vector of infectious and toxic hazards among school-aged children; food contact with unwashed hands can be a source of diarrhoea pathogens. The widespread presence of intestinal parasites impairs the absorption and digestion of nutrients, thus calling for environmental prevention of parasite cycles, improved sanitation, hygiene education, and eventually community deworming.17 Handwashing should therefore be combined to nutrition education. The Ministry of Basic Education recently declared a joint call to Action for WASH (Water, Sanitation, and Hygiene) in schools in collaboration with the Ministry of Public Health and UNICEF.
The NGO NOODLES (Nutrition & food safety and wholesomeness. Prevention, education and research network, www.noodlesonlus.org) highlighted how schoolchildren in Cameroon are at risk of foodborne diseases due to poor hygiene and sanitation in schools’ environment and canteens. Indeed, children have the right to be in a school that provides safe water, sanitation and hygiene education. Diseases prevention will considerably improve if proper handwashing, healthy eating and dietary habits are instilled from an early age. Moreover, since oral hygiene positively affects mastication, dietary diversity, and nutrition,23 oral health should be promoted simultaneously with nutrition education and handwashing. In North-West schools 26.7% of children (12-13 years old) had gingivitis; parents, dental professionals, and teachers were the main sources of instruction on oral care.24
The purpose of the present study was to:
-
combine nutrition, handwashing, and dental care education to improve the health literacy of schoolchildren,
-
engage the school system in the promotion of healthy food choices and hygiene,
-
assess and analyse children nutrition-related knowledge-attitude-practice (KAP), and gain insight on children and school community determinants of health.
The applied methodology is inspired from the FAO KAP approach and guideline.25 KAP studies are intended for two main purposes: a) gain information in situation analysis that can feed the design of more extensive interventions and b) evaluate the impact of nutrition education interventions. KAP indicators include: i) understanding of key concepts and facts, ii) attitude towards nutrition related health problems, iii) observable behavior and practices, including the frequency and amount of diverse foods.
METHODS
Location and flow-chart of activities
Yaoundé, the second largest city in the country, is a 180 km2 area. It is located in the Centre Region, in the Department of Mfoundi with following coordinates: 3°52’N 11°31’E. The town of Yaoundé, capital city of Cameroon, was used as study area because it represents a micro-environment where almost all tribes, different trends in consumers’ behavior and household groups are found. The Yaoundé Urban Councils are shown in Figure 1.

This pilot project on nutrition, handwashing and dental care education developed from September to December 2017. It followed 4 main phases: i) managerial issues: administrative clearance; coordination within the territory; ethical clearance; selection of schools; enrolment of schoolchildren; informed consent; ii) engagement of the school community/school environment: sensitisation and demonstrations with parents and teachers; donation of equipment and materials; iii) frontal education: 6 modules course; pre- post-assessment; iv) evaluation of outcomes: statistical analysis; long-term audit (December 2019).
Administrative clearance and coordination within the territory
The Ministry of Public Health (in charge of nutritional education and health), the Ministry of Basic Education (in charge of primary schools) and the Ministry of Mines and Industries (in charge of activities of the national secretariat of Codex Alimentarius and food safety) were informed along with the regional offices of UNICEF (WASH program), African Union, and World Food Program. The project was reviewed and officially approved by the Ministry of Basic Education under the code 131/1464/L/MINEDUB/SG/DSSAPPS/SDSS/SHP.
The celebration of the 3rd edition of the African School Alimentation day (March 1st, 2017) and the Global Hand Washing day with the theme “Clean hands for all” (October 15th 2019) were exploited to increase awareness and foster advocacy. Video clips (max 30 minutes) in French with subtitles in English were disseminated along with the project report to the school administrations and stakeholders.
Ethical clearance
Ethical clearance was granted by the Centre for Research and Graduate Studies in Life Health & Environment Science at the Biotechnology Center, University of Yaoundé, Cameroon. The ethical clearance required parental approval during the phase of enrolment of children.
Selection of participating schools
In preparation of the academic year 2017-2018 (starting in September), letters of information about the initiative of nutrition and hygiene education intervention were sent to the headmaster of randomly selected schools among those registered under the Ministry of Basic Education in the different Yaoundé urban councils. Follow up meeting where organised with headmasters of respondent schools to decide the enrolled ones. Schools in the north-west and south-west of the country dropped out due to ongoing strike. Children attending public school are generally much more than those attending private schools in Cameroon. Since they could not host the course within the two school shifts (7:30am-12:00am; 12:00am- 5pm), public school could not engage in our study. Private schools in the Centre region did engage in our study, with their limited number of children within the age group. The NGO NOODLES and each enrolled school signed the Agreement, based on mutual expectations and common objectives. In particular, the agreement focused on: the calendar of education teaching modules, 1 hour/week education module per 6 weeks, grouping of children according to age, follow up activities including periodic audits, donation of handwashing equipment, guarantee on appropriate use and maintenance of donated equipment and compliance with related daily good practices.
At the end of September 2017, four bilingual primary private schools in different Yaoundé councils enrolled in the study, namely the Bright Minds School, the Omega School, the Saint Theresa school, and the Tebah school (Figure 2).

Enrolment of children: sampling procedure
Following the agreement with the school, a convenience sampling method was used to enroll 71 respondents as recommended for pilot studies26. Respondents were primary school children (7-12 years old), of which 36 were females (50.7%) and 35 were males (49.3%), with mean age 9.5±0.2. In particular, 13 children (9.0±0.3 years old) were recruited from the Bright Minds school; 33 children (10.0±0.2 years old) from the Omega school; 15 children (10.5±0.2 years old) from the Tebah school; children (10) enrolled at Saint Theresa school were the youngest (7.2±0.2). Consent forms were distributed to the parents/caregivers and children; all caregivers and children gave their permission to publish pictures.
Engagement of the school community/school environment
Kick off meeting. Between September and October 2017, the NOODLES team organised the kick off meeting with Parent Teacher Association (PTA) in the four enrolled schools. During such meeting, details of the project (including objectives, activities and calendar) were clarified to teachers and caregivers. During the kick-off PTA meeting, parents requested advices on ways to elaborate nutritional balanced menu for children with the very low income they have. They also asked how to properly package and prepare meals for transport to school.
Donation of toolkit policy. The Cameroonian toolkit policy to ensure safety, quality, and nutritional value of packed lunch, and context specific minimum standards for WASH in schools based on UNICEF/WHO guidelines were presented. Hard copies of the Cameroonian toolkit policy were donated to each school to enable the consistent approach to the intervention and facilitate the implementation.
Donation of plasticised communication posters. Plasticised communication posters on handwashing, food pyramid and weekly diet plan were donated for exposure in the 4 schools.
Donation of WASH equipment and disposable materials. Since nutrition education is a combination of theories and actions facilitating the adoption of appropriate behaviors and practices, a set of equipment and disposable material was donated to each school, including 3 handwashing stations, 3 bowls, 3 liquid soaps and 10 package of paper towels. Further to the initial set of material, the following material was used during the education courses in the 4 schools: clean water, tooth brush, tooth paste, dental floss, game puzzles, apples, samples of local crops.
Engagement of parents/caregivers. Caregivers/parents accepted to collaborate with the NOODLES team. One caregiver/parent per child, i.e. the person (aged above 21 years) preparing the child’s lunch, agreed to record pre- and post- education child’s food preferences.
Engagement of teachers. Teachers agreed to carry out daily open discussion with children on safety, quality and nutritional value of meals based on packed lunches, with great emphasis on respect to families and children. Teachers made puzzles from the food pyramid and the children organised food information that way. Teachers also agreed to daily monitoring appropriate handwashing and oral hygiene. Observation by teachers of daily meals packed by caregivers for children during the same period (e.g. monotonous or diversified diet with e.g. rice, fish, vegetables or fruits; frequency; portions) allowed the assessment of daily practices at home.
Engagement of school canteen operators. One school (Omega) had a school canteen; canteen operators accepted to participate to the demonstrations on nutrition-related good practices and training on the use and implementation of the toolkit policy.
Engagement of school system. The proactivity/responsiveness of the school system, i.e. the community-based sustainability of the intervention towards the implementation of a safer environment (e.g. handwashing devices and hygiene and sanitation practices) and good practices for safer and nutritious meals at school was verified in a long term audit (24 months later, December 2019).
Demonstrations on WASH-related daily good practices. WASH-related daily good practices, e.g. pouring clean water in the handwashing stations (Figure 3) and logistics, were held with the school communities.

Sensitisation and demonstration on nutrition-related good practices. Sensitisation and demonstration sessions (3hs, twice) were held to sensitise teachers, caregivers/parents and canteen operators (when available) during PTA meetings (Figure 4). Sessions mainly consisted of: practical demonstrations on safety (chemical risks), hygiene (microbial risks) and nutritional values; water sanitation; good practices in food storage; appropriate packaging and transport of meals to school; organisation, sanitation and hygiene of kitchen and waste system27,28; organisation of cost-effective school feeding program. Traditional local recipes (e.g. millet cake, poi doughnut, banana millet bread, Figure 5) based on local crops were cooked. Weekly menu was proposed to parents, and recipes were given (printed copies) on how to cook and conserve certain foods with local ingredients (Figure 6).



Combined nutrition, handwashing and dental care education
The combined nutrition, handwashing and dental care education course (English/French) was repeated twice in each school by two members of the NGO. A third member was in charge of taking pictures and making video for narrative prevention reportages,29 possibly highlighting behaviors deserving improvement.
The course covered the following 6 modules (1 hour/week, 6 weeks) during lunch time:
-
basic foods groups using colors, and relationship between nutrients and their function for well-being: children list at least one specific function of each nutrient class;
-
food sources for specific macro and micronutrients (children draw their usual breakfast and their favorites foods). This module is delivered in the form of interactive game;
-
the sense of taste (salty, sweet, sour, bitter). Pictures of many food items from different food groups were proposed to children, asking them to cut out and classify e.g. those high in fiber, fat, sugar, salt, or mineral;
-
building of a food pyramid (game puzzle) for balanced nutrition and portions using commonly eaten food items. Children start drawing it at home with their parents, and bring it at school for discussion;
-
dental care (best practices in teeth brushing);
-
handwashing after toilet use, before meals and after recreation in the open space.
Questionnaire
Following the FAO approach and guideline,25 the individual and community nutrition-related KAP were assessed and analysed with a multiple-choice questionnaire before (baseline assessment) and after (end-line assessment) the nutrition, handwashing and dental care education course. The questionnaire was preliminarily discussed with 14 mothers of children aged 7-12 years old to verify the correct understanding of questions, identify eventual bias in answers, estimate the test duration and receive the caregivers’ feedback. Some parents complained of time constraints to fill in the forms. After a debriefing, the final questionnaire contained a total number of 52 questions, organised in 10 categories (Figure 7). Further to socio-demographic factors (age and gender of children), the categories were: nutritional information (2 questions), eating habits at school (2 questions), nutrition knowledge (8 questions), food choices (4 questions), nutrient sources (3 questions), practices (9 questions), attitude (8 questions), dental care (4 questions), and handwashing (10 questions). Questionnaire section-based and overall scores, ranging from 0 to 1, were used as indicators. Scores represented the number of right answers by the respondent over the total number of questions. Scores were analysed using paired z- and t-tests with SPSS 23.0 for windows.

To assess their knowledge, children were asked to choose their answer (True or False) among 3 to 6 possible answers depending on the category. For instance, they replied to questions on salty food (are they good for health or not), the importance of food for growth, symptoms of foodborne diseases, etc. They were also asked to report i) foods that they usually have for lunch; ii) the kind of mixture; iii) the number of portions and fruits; iv) how often fruits, milk and vegetables are included. According to its definition, “attitude” towards a practice depends on perceived benefits of the practice, perceived susceptibility to the underlying problem, perceived severity of such problem, perceived barriers to the practice (e.g. resources, but also tradition-rooted habits and preferences, and self-confidence).25 To assess their attitude, children were asked to reply (I agree, I do not agree, not at all) on issues like: “breakfast is very important”, “I need to eat a balanced diet to stay healthy”, “I need to eat a variety of foods daily”, “I must study nutrition and food safety to stay healthy”, etc. Questions on the frequency of teeth brushing, relevant tools, experienced teeth problems, and experience of the visit by dentists depicted the scenario of dental care. Questions related to handwashing focused on how hands are washed; whether hands are washed after toilet use, after schools, before the meal, after sneezing, after playing, and if usually hands are washed at schools.
Data quality and statistical analysis
The internal consistency of the questionnaire was assessed by Cronbach’s Alpha. Pre- and post- questionnaires were verified before the assessment to avoid errors, omissions, and incongruous data. Double data entry avoided data entry errors from the questionnaires (pre and post) in the Excel sheet.
Socio-demographic characteristics were summarised using frequency and percent distribution for gender, mean and standard deviation for age. The nutrition scores (NS) of the 9 categories were calculated similarly to the Consumer Satisfaction Index (CSI)30; partial NS for separate sections were calculated using the following formula:
NSj = Rj/ TQ
Where:
Rj: number of right response answers in each section
TQ: total number of questions in the section.
The overall NS was calculated using the following formula:
NS=n∑k=1NSjwj
Where:
NSj: partial NS for the j section,
Wj: weight (importance) of the j section (equal to 0.143, i.e. 1/7 for all sections).
Nutrition scores were presented in proportion ± standard deviation and categorised as follows: weak (0.0-0.49), average (0.5-0.69) and competent (0.7-1.0) according to the grade assessment applied in primary education in Cameroon.
Paired t-tests with SPSS 23.0 for windows were used to evaluate outcome variables at the significant level of 0.05. Partial scores were compared using two-tailed paired t-test and the overall scores using two-tailed z-test. Scores were compared using a lower one-tailed paired t-test using the Bonferroni adjustment.
RESULTS
Internal reliability of the questionnaire
The minimum requirement for internal consistency is 0.7.31 The Cronbach’s alpha of the questionnaire used in this study was 0.722. The questionnaire exhibited a high internal consistency and demonstrated that the items in the questionnaire were all reliable in measuring food-related habits (food choices, nutrients sources, dental care, handwashing) and nutrition KAP. The questionnaire response rate after the intervention was 100%.
Impact on nutrition knowledge, attitude and practices
Knowledge. With the exception of Tebah school (where almost nobody ever heard about it), most children in the schools have previously heard about a healthy diet from friends, nurses and teachers. At Omega school, all children said to have heard about a healthy diet by the canteen worker. According to our criterion, children at Tebah school had a weak level of knowledge at baseline, whereas children at Bright Minds School and Saint Theresa schools had an intermediate level and children at Omega school were competent. After the intervention, a significant improvement was found at Tebah school, where children increased their competence from weak to intermediate level (Table 1).
Attitude. At baseline, children at Bright Minds school were competent, while children at Omega and Saint Theresa schools were intermediate, and weak at Tebah school. A significant effect on competence was obtained at Tebah school (from weak to competent) (Table 1). Noticeably, a drop in the score was obtained at Bright Minds, where the level decreased from competent to intermediate.
Practices. At baseline, practices were weak in all sampled schools. After the nutrition education, the competence level increased from weak to intermediate at Tebah school. At Saint Theresa school, the level remained weak but with a significant increase in the score (Table 1).
Food choices. Competency in food choices was high since the beginning, except at Tebah school. After nutrition education, the situation significantly improved at Tebah, where children increased from weak up to competent (Table 2). Whether they purchase them at school or bring them from home, children more frequently eat certain foods. Before the education intervention, more than 70% of the children brought lunch from home such as bread and fried eggs, doughnuts, fried plantain and cake, buttered biscuits, bread and chocolate. Providing children with fruits and drinking water for their meals was not a common practice. An increase in the proportion of fresh fruits, enriched cakes and doughnuts made with local crops, such as banana millet cake and soya beans doughnuts, was observed after the education course.
Nutrient sources. The competencies of children at Tebah and Saint Theresa schools remained weak (with some improvement at Tebah); children at Bright Minds school remained intermediate in level (Table 2). Noticeably, children at Omega school decreased their level from competent to weak.
Impact of the nutrition-related hygiene education
Dental care. Competences were weak in all schools (Table 3) and remained weak, except at Tebah school, where scores increased significantly, and children moved to intermediate level.
Handwashing. At baseline, the competence of children at Omega and Tebah schools was weak, while the competence of children at Bright Minds and Saint Theresa schools was intermediate. A significant increase was gained in three schools; scores also increased at Bright Minds school. Children at Omega school developed an intermediate competence, whereas children at Tebah, Saint Theresa and Bright Minds schools became competent (Table 3).
Overall scores
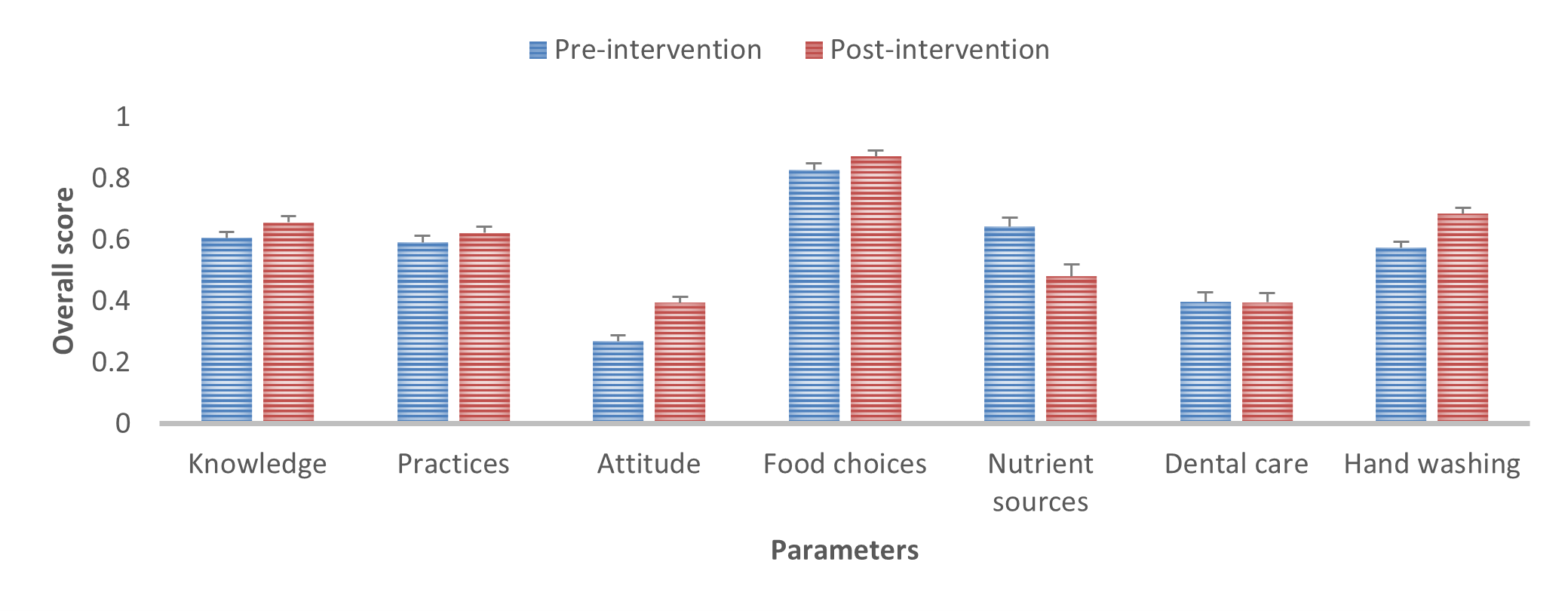
Overall, the intervention did not show significant effect on knowledge (overall average score 0.63, P=0.082), practices (score 0.61, P=0.318) and dental care (score 0.40, P=0.968) (Figure 8). Nutrition attitude was considerably affected, with an overall score increasing from 0.27 to 0.40 (P=0.001). Food choices were also positively improved, with an overall score shifting from 0.83 to 0.87 (P=0.001). Handwashing was substantially improved, with an overall score changing from 0.57 to 0.68 (P<0.001). Competence in nutrient sources was negatively affected (from 0.64 to 0.48, P=0.001).

Results by gender and by age
The stratification of the group of children by gender (Table 4) revealed that:
-
girls had lower knowledge respect to boys (weak vs intermediate)
-
both girls and boys were competent in food choices but intermediate in recognising nutrient sources
-
decreased competence (intermediate to weak) in nutrient sources observed in Table 2 were more common in girls
-
both girls and boys significantly increased their score in handwashing, and boys increased to a competent level
The stratification of the group of children by age (Table 5) revealed that:
-
children over 9 years old had lower knowledge and practices with respect to children below 10
-
children over 9 years old significantly benefited from the course (increased knowledge, attitude, practices, food choices, handwashing), with the exception of nutrient sources (drop from intermediate to weak)
-
children under 10 years old significantly improved in practices and handwashing while significantly decreasing their score in dental care. Their improvement in knowledge, attitude, food choices and nutrient sources was insignificant.
Sustainability of the outcome
The long-term audit on the impact of the education intervention over time reported good sustainability of the outcome. Handwashing stations were found in good conditions and daily used, while the PTA continued to provide funds for disposable materials such as paper towels, liquid soap, clean water, toothbrush, toothpaste and dental floss. A remarkable nutrition education promotional activity spontaneously emerged at the Bright Minds School during the Global Hand Washing day in 2019 (Figure 9). The Saint Theresa school exploited the recipes learned during the nutrition course (e.g. soya beans doughnuts) to ensure children have a regular intake of proteins (Figure 10).


DISCUSSION
At baseline, children could correctly answer more than half of the 52 questions, except at Tebah school. Children at Tebah school had a minimal previous discussion at home, at school, at the hospital, or elsewhere on the course-related issues. This aspect corroborates the socio-cultural environment as the main factor affecting healthy eating habits and hygiene practices, as already observed in Chad.32 Tebah school is characterised by overcrowded classes. Children generally belong to families with insufficient financial resources. Although socio-cultural parameters (such as family and social network, cultural practices and food taboos, social structures, public policy, and physical environment like food availability and built environment) were not included in the questionnaire, they emerged as possible impacting factors. While most of the children (70-100%) in this study brought their lunch from home (Figure 11) and 22% of children at Bright Minds school purchased their lunch at school, 72% of children at Tebah school declared not to have lunch at all (Figure 11). More generally, the role of economic environment (e.g. resources; informational environment like advertising; media; classroom curriculum; health and nutrition education intervention) on attitude has emerged. The four schools showed significant differences based on a different perception of diseases prevention and different personal attitudes plausibly associated with the social-economical level of families, age of teachers (older teachers acquire more nutrition knowledge), years of schooling before primary school, better school environment.33 In particular, the education course significantly affected scores of three out of four schools (Tebah > Saint Theresa > Omega), while no significant effect was observed at Bright Minds school. Indeed, as already proven by a survey developed by the NOODLES NGO in Cameroon, preventive medicine is a matter of both awareness and affordability.11

Sensitisation and demonstration meetings with PTA stimulated the engagement of caregivers in improving the safety, quality and nutritional value of meals while contributing to a more responsive school environment. The provision of materials and equipment coupled positively with efforts by the school community towards sustainable habits’ change. For instance, the provision of materials for teeth hygiene significantly improved dental care of children at Tebah school (Table 3) while we know that children’s dental health is significantly associated with oral health literacy of caregivers.34,35 The improvement in handwashing practices in the four schools was drastic, independently of gender and age, probably due to multiple daily practical demonstrations on proper handwashing and the availability of handwashing devices and disposables (Figure 12). Handwashing with soap is critical in reducing exposure to pathogens and respiratory and diarrheal diseases,36 and therefore in reducing school absenteeism. However, the gap between knowledge on the importance of handwashing and actual handwashing practice, especially with soap, generally persists37,38 probably due to the absence of appropriate water sources, essential equipment and a supportive environment.

Nutrition education may be crucial in developing healthy behaviours for improved nutritional status,39 possibly impacting cognitive abilities also.13 Conversation on packed lunches for safety, quality and nutritional value facilitates parents in making appropriate changes to meet the school standard; we also found that the application of the toolkit policy enabled the schools to have a consistent approach to this intervention. While the nutrition attitude and food choices improved in the four schools, interestingly the nutrition education failed in improving the understanding on how to identify nutrient-rich foods. This was probably due to a poor understanding of the concept of nutrient sources. The overall score in nutrient sources showed a statistical decrease mainly attributable to girls and older children (above 9 years old). This finding could be partly linked with the general trend towards unhealthy food choices (e.g. energy-dense foods, sugar-sweetened beverages) in children in sub-Sahara Africa.17 A recent survey conducted by the NOODLES organisation in Cameroon highlighted how retailers claim failure to sell fruits due to poor consumers’ awareness of the healthy value of fresh fruits and vegetables.8 Despite the low price and easy access, consumers’ demand of fresh fruit and vegetables is low. Poor dietary habits seem associated with a lack of understanding of nutrient sources,40 and therefore more a matter of awareness than affordability.
To our knowledge, this has been the first education course including elements of food safety in developing settings. Foods can be contaminated by a large range of chemicals, from those intended for use in agriculture and zootechny (e.g., residues of veterinary drugs and pesticides), to environmental contaminants (e.g. toxic metals) and natural toxins (e.g. mycotoxins).41 Moreover, when good practices are not known, toxic by-products can be formed during cooking.27,28 Direct documentation in situ can disclose overlooked real-life bad practices.29 For instance, images captured during this education course highlighted the unsafe daily habit of wrapping food in newspapers; it is known how newspapers release toxic substances from the printing inks.29 Not to mention the water stored in plastic bottles, which release plasticisers when exposed to the sun. The relevant risk of daily low dose exposure to toxic substances was discussed with caregivers and canteen operators, and communities turned out as proactive towards empowerment on healthy habits and good practices.5
The impact on nutrition knowledge, principally in 2 out of 4 schools (Tebah and Saint Theresa), is particularly significant if we consider that this education course offered less than the 5 hours of required nutrition education per year. The course was far below the 40-50 hours required during the school cycle to connect knowledge and practice and affect behaviour change.42 Our course highlighted how connecting knowledge and practice is a challenge and requires behaviour and attitude change43; it also confirmed how the capacity of understanding the effect of food on the body increases with age.
Concerning the specific purposes of the present study, we can observe the following. With nutrition education, hygiene education (handwashing and oral care) can be profitable. One limitation of the present study was the small group of children enrolled in each school, mainly due to the limited number of children (7-12 years old) attending a private school in the sampled area. A larger participating group will be most likely obtained in a subsequent education intervention through a sounder preliminary preparatory plan started well in advance in the public school system.
While the level of engagement of the school system was satisfying in the present study, the next education intervention will include an initial sounder plan. The initial plan should: i) enforce the school nutrition policy (i.e. a more profound training of teachers on the implementation of the policy toolkit), ii) incorporate nutrition, hygiene and food safety education in the school curriculum (whole school cycle), iii) design a more class-oriented nutrition education (e.g. multiple learning sessions in the day or week). This will encourage the stable involvement of all the members of the school community, facilitate more targeted programs (e.g. schools in need of more material; children in need of simplified or upgraded course), and allow charting the impact over time. The education module on nutrient sources will require specific efforts and communication strategy.
Finally yet importantly, nutrition and hygiene education can improve knowledge but not necessarily translate into healthy behaviors.13 Indeed, knowledge may have a limited impact in the absence of a facilitating environment (pre-requisites to health), including appropriate access to safe water and sanitised toilets.
CONCLUSIONS
Despite some advancements in regulations by the Ministry of Basic education and Ministry of Public Health, more efforts are needed to update and enforce the proper nutrition of children at school. Steady progress in safe and healthy nutrition at schools will benefit from the coordination with other initiatives contributing the UNICEF/WASH programme and the national action plan and, in some circumstances, the WFP. Structural sustainability of the intervention cannot disregard food safety in public health training programs and training on nutrition education in academic curricula (currently absent in the eight states universities in Cameroon). Knowledge in action requires an improved academic attitude towards translational research, from theory to real-life and communities.
Acknowledgements
The authors are grateful to the school managers, the teachers, the caregivers and the schoolchildren who have accepted to take part in this education course. We are grateful to the Ministry of Basic Education and the Ethical Committee of the Centre for Research and Graduate Studies in Life Health & Environment Science at the Biotechnology Center, University of Yaoundé, Cameroon for reviewing and approving the project.
Funding
The University of Tuscia (Viterbo, Italy) funded this project under the agreement (2017-2018) with the NGO NOODLES Cameroon.
Authorship contributions
CF wrote and presented the project proposal for the grant. PFY coordinated the pedagogic activities; PFY and FM organised the pedagogic material. PFY, JTS, CS, and ASK implemented the courses in the schools. BS and FM made statistical analysis. GBP handled administrative and managerial aspects. GBP and BS drafted the project report, and EF revised it. CF wrote the final paper on the base of the full range of work done.
Competing interests
The authors completed the Unified Competing Interest form at http://www.icmje.org/disclosure-of-interest/, and declare no conflicts of interest.
Correspondence to:
Chiara Frazzoli Ph.D.
Department of Cardiovascular and endocrine-metabolic diseases, and ageing
Istituto Superiore di Sanità
Via Giano della Bella 34, 00162 Rome, Italy
[email protected]