

Therapeutic opioids (eg, morphine) are listed as Essential Medicines by the World Health Organization (WHO) for a wide range of clinical problems.1 Opioids are a key aspect of the WHO’s widely-used three-step pain ladder and are a primary treatment for acute pain and for cancer pain.2 Opioids also are indicated in common clinical scenarios such as childbirth,3 acute musculoskeletal pain,4 trauma,5 peri-operative care6 and, in low doses for chronic breathlessness.7 Additional to physical suffering caused by lack of pain relief, clinical outcomes are worsened (e.g. heightened risk of post-operative pneumonia8) and socio-economic prospects of individuals and families are jeopardised (e.g. risk of poverty due to inability to work due to uncontrolled pain9). These circumstances have led to calls for access to pain relief as a basic human right.10
Additional to clinical benefits, therapeutic opioids are formulations with addictive properties and the potential to cause harm.11 Inappropriate prescribing of therapeutic opioids can lead to dependence and addiction, making use of evidence-based clinical guidelines, extremely important for safe prescribing and use. Due to potential risks of inappropriate use, opioids are controlled substances, subject to international and national regulation and there is ongoing debate regarding how to ensure balanced policies for access and safe use of controlled medicines.12
The International Narcotics Control Board (INCB) has overseen international drug control since 1968 with the dual remit of restricting illicit production or use of controlled substances, whilst enabling access for clinical purposes.13 It is a quasi-judicial organization and the only United Nations (UN) agency with powers of enforcement.14 The INCB aims to oversee the implementation of international drug conventions, ratified by UN member states.15 International drug laws aim to restrict illicit production and use of harmful opioid substances and ensure appropriate access to opioid formulations for clinical and scientific purposes.13
Two dichotomised global public health crises are present under the stewardship of the INCB.
First, there is a continuing crisis relating to addiction and misuse of opioids, primarily in North America and Western Europe.16 In the United States, drug overdose is now the leading cause of injury death.17 A complex array of factors have led to this situation.18 The United States government attributes the rise in prescription opioid misuse to factors including: lower prices, aggressive marketing by opioid manufacturers, changing prescription practices and inadequate controls.19 Pharmaceutical companies and even physicians now face criminal lawsuits for advertising and prescribing practices related to opioids.20 Despite the emphasis in the public discourse on prescription opioids, most opioid-related deaths are still caused by illicitly-obtained, not prescribed, opioids.21
Second, and the primary concern of this paper, is the larger public health crisis relating to the billions of people globally who do or will suffer unnecessarily due to lack of any access to any opioid analgesia, despite their relatively low costs.22
In terms of ensuring access to controlled substances for clinical purposes, the INCB uses the ‘Estimated Requirements for Substances under International Control’ system to oversee implementation of international drug laws. Each year, countries estimate their national requirements for therapeutic opioid use, which places an upper limit on stocks and trade.23 Should countries fail to comply with the Estimates system, the INCB may call on governments to take remedial actions, or even “recommend to Parties that they stop importing drugs from a defaulting country, exporting drugs to it or both.”24 The consequence of governments failing to comply with the Estimates system may therefore be INCB-endorsed further restriction of access to Essential Medicines.
Under the estimates system, there are huge inequities in access to opioids between countries and most people who may benefit from their use do not have any access.25 The INCB reports that:
“In 2018, 79 per cent of the world’s population, living mainly in low- and middle-income countries, consumed only 13 per cent of the total amount of morphine used for the management of pain and suffering, that is, 1 per cent of the morphine manufactured worldwide” [INCB, 201926].
In the lifetime of the INCB, illicit opioids have become a security issue in many parts of the world, rather than a political or social issue, with a consequent global increase in incarceration rates for misuse of drugs.27 This is relevant to the present paper as key barriers remain which continue to limit legitimate access to those in need. Barriers include: over-regulation, lack of prescribing knowledge of physicians and ‘opiophobia,’ or fear of opioids due to the threat of legal action for mis-prescribing.28,29
After sixty years of the regulation of opioids by the INCB, a complex situation prevails of two ‘opioid crises’, where licitly produced and illicitly produced opioids may be accessed for both licit and illicit purposes. Few nations worldwide have been able to successfully implement international drug conventions with national policies that achieve the appropriate balance between restricting inappropriate access and ensuring appropriate access to therapeutic opioids. It is therefore timely to review the role played by the INCB in limiting illicit production and use while promoting safe and systemic access to opioids for medical, scientific and research purposes. We investigate the regulatory climate promoted by the INCB as represented through the language used about opioids in a representative sample of six Annual Reports each one a decade apart, from 1968-2018.
METHODS
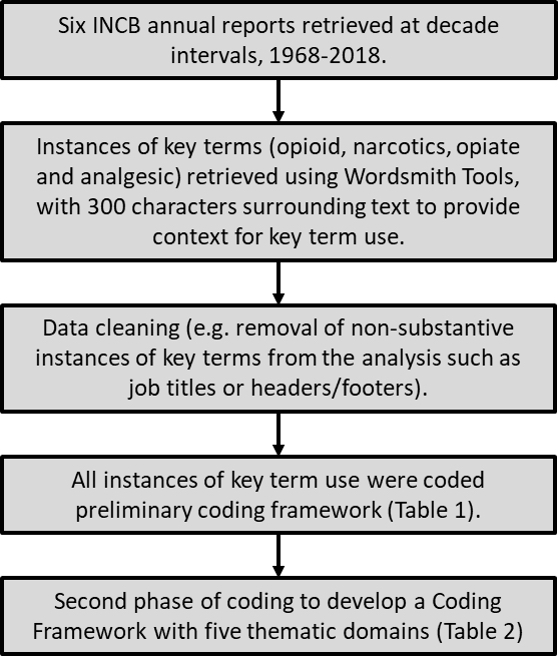
We conducted a systematic critical analysis of a representative sample of INCB annual reports using corpus linguistics as a method of document analysis.30 Use of quantitative and qualitative methods allowed investigation of our primary interest in how language is used by the INCB in relation to opioids, seeking to identify the relative emphasis on licit and illicit issues, and whether this has changed over time. The study:
- Identifies key terms used by the INCB relating to therapeutic opioids;
- Quantifies the proportional prevalence of key terms within annual reports and how this has changed over time;
- Describes key discourses of the INCB relating to opioids; and
- Quantifies the proportional prevalence of key discourses within annual reports and how this has changed over time.

Document sampling
The INCB is required to publish an annual report which provides a comprehensive account of the global drug situation.31 Further publications include: 'Precursors and chemicals frequently used in the illicit manufacture of narcotic drugs and psychotropic substances’ and technical reports on narcotic drug use/production and estimates of legitimate requirements of each country. Although such reports are relevant to opioid analgesia, the INCB lists the production of an annual report as part of its Mandate and Function and may be considered as the key vehicle to connect the organisation with policy makers, law makers and the public in relation to accountability. We therefore selected INCB annual reports as the most appropriate lens through which to investigate the INCB’s organisational priorities.32
The first INCB annual report was published in 1968. We included annual reports at decade intervals (1968-2018) as a means of tracking representative changes and developments in the discourse of the INCB since its inception.33
Key terms
We consulted the US National Library of Medicine website to extract historic Medical Subject Headings (MeSH) of words related to opioid analgesia. All relevant terms (opioid, narcotics, opiate and analgesic) identified were included as key terms.
Data cleaning
INCB reports are publicly available. Annual Reports were ‘cleaned’ by removing non-substantive instances of key terms from the analysis such as job titles or headers/footers. Appendices, explanatory notes and glossaries were also excluded. We imported six Annual Reports into Wordsmith Tools v6.0 (Scott, 2012, United Kingdom) for data analysis.34
Analysis
Using Wordsmith Tools, frequencies of key word usage were retrieved as Wordlists. Wordlists incorporated use of plurals (e.g. opioid/opioids) and relevant synonyms (eg, analgesia/analgesic). Frequency of key term use and overall Annual Report word counts were extracted. Frequencies of keywords per 1000 words were calculated to identify the relative prevalence of our key terms.
A priori coding framework
An a priori coding framework was developed by preliminary coding using an iterative approach (Table 1). Key terms are used interchangeably by the INCB and were coded as either a description of clinical (therapeutic) use, illicit use, or both.
All instances of key term use were coded independently by two researchers (JC, BF). Three hundred characters surrounding key terms (opioids, opiates, analgesics, narcotics) were retrieved to allow coding in context using an iterative approach to develop themes.
Agreement between reviewers was 85% and conflicts were resolved with discussion between the study team. Further independent ‘free coding’ by two researchers (JC, BF) of keywords in context took place to develop a preliminary seven-issue coding framework. After initial codes were assigned, the framework was refined through discussion as a study team in to a five-issue / three domain framework, ahead of further piloting and finalisation of the coding framework (Table 2).
Our coding framework reveals the key thematic discourses of the INCB and the relative attention given to each. We report frequencies per-1000 words of themes and key terms, aggregated and by decade.
RESULTS
Five themes were developed within three domains (Table 2).
The developed thematic categories account for key term use in the context of illicit and licit production, distribution, supply and demand for opioids, as well as discourse around national and international drug policies and enforcement agencies.
Quantitative analysis of word frequency within our sample, showed that key terms appeared in the six Annual Reports a total of 1376 times. Proportionately, key terms appeared in INCB Annual Reports most commonly in relation to the Illegal Drug Trade (0·14 per 1000 words), followed by Policy, Enforcement, Definitions and Context (0·11/1000 words) and, Estimates of licit need, use and related topics (0·09 per 1000 words) (Figure 2).

There are fewer instances of Access to Opioids for a Therapeutic Use (0·06 per 1000 words), lower than key term use relating to Abuse and Dependency (0·08 per 1000 words).
There has been a sustained emphasis in the discourse relating to Abuse and Dependency, Policy and Enforcement, Definitions and Context and, the Illegal Drug Trade since 1968 (Figure 3). In every single year, discourse related to the Illegal Drug Trade is demonstrably more prevalent than Access to Opioids for Therapeutic Use.

The spike around Policy Enforcement, Definitions and Context in 1968 is arguably due to this being the first annual report of the INCB, with much discourse directed towards the stated goals of the INCB to implement the Single Convention on Narcotics.
Discourse in relation to Estimates of Licit Need is the only clinical theme in 1968 and has a high point in 1978, after which, overall reference decreases decade on decade. There was noticeably increased attention upon issues in relation to Access to Opioids for a Therapeutic Use in 2008, which is otherwise low.
‘Narcotics’ is the key term most commonly used within all INCB annual reports within the sample (S1 in the Online Supplementary Document). The proportional use of ‘narcotics’ decreased since a high point in 1968, consistent with the focus upon Policy reported in Figure 3. From very limited use of ‘opiates’ in 1968, this increased in 1978 before decreasing and remaining consistent until 2018.
There is almost no mention of ‘analgesia / analgesics’ until 1998 and limited use at subsequent time points. This is consistent with the minimal discourse relating to symptom management identified within reports regarding Access to Opioids for Therapeutic Use. There has been noticeably increased use of ‘opioids,’ since 2008. Given the increased discourse around Abuse and Dependency since 2008, it seems likely that increased use of the term ‘opioids’ relates to what has been termed the opioid crisis in relation to overuse and abuse of narcotics in a handful of high-income countries.
DISCUSSION
Our systematic critical analysis of INCB Annual Reports using methods of corpus linguistics suggests that the INCB prioritises the prohibition of production, trade and, illicit use of opioids over their enablement for clinical purposes. This approach has been in evidence since the first INCB report in 1968 and remains in 2018. Discourse around The Illegal Drug Trade and Abuse and Dependency is prevalent within all reports in our sample. By contrast, little attention has been paid to Access to Opioids for a Therapeutic use. Of concern, discourse relating to Estimates of Licit Need, Use and Related Topics has also decreased over time.
Under the Estimates system, millions of people with present clinical need, predominantly in low- and middle-income countries continue to lack any access at all to essential opioid medications. Key components of the Estimates system are shown in S2 in the Online Supplementary Document. Importantly, the INCB draws a distinction between ‘need’ and ‘requirements’ for controlled substances. ‘Need’ relates to an estimate based on the size of the population, whereas ‘requirements’ relate to quantities that health and law enforcement systems are perceived to be able to manage safely in the context of existing health infrastructure. The INCB places the obligation upon nations to devise their method of estimating need based upon one of three approaches reported in Box 1.
There is no evidence base cited for any of these three approaches to estimating the annual needs or requirements for opioids at the national population level. Each approach is based upon historic data and practices (which most commonly have guaranteed inadequate access to therapeutic opioids for licit purposes. Method A appears to encourage a path towards ongoing inadequate access, whereby consumption estimates cannot exceed usage in previous years. Method B is reliant upon there being any examples of appropriate therapeutic opioid availability in standard health-care facilities. Method C is reliant upon morbidity estimates from countries facing serious challenges in accurate disease surveillance. None of these processes appears responsive to changing clinical guidelines or future needs.

In the absence of validated guidelines, academics have adopted alternative measures for opioid consumption. For example, the Lancet Commission used the Distributed Opioid Morphine Equivalent (DOME), an approach which assess the quantity of opioids available for prescription in countries, though the document still offers no method of assessing total need. Statistical approaches consider the adequacy of therapeutic opioid consumption by measuring adequacy of nations’ consumption in relation to that of twenty countries with high Human Development indices which are used as comparators.40 Whilst such efforts further the conversation, none of these approaches have been evaluated and do not inform governments submitting their estimates of requirements to the INCB.
INCB reports contain detailed country reports, including data on ‘seizures of opioids’ from illicit channels. However, no data are published by the INCB relating to estimated 'needs’ for therapeutic opioids. Only quantities for ‘requirements’ are published. This is in spite of huge variation between countries with similar populations in terms of estimated requirements.41 What then is the gap between needs and requirements for countries around the world?
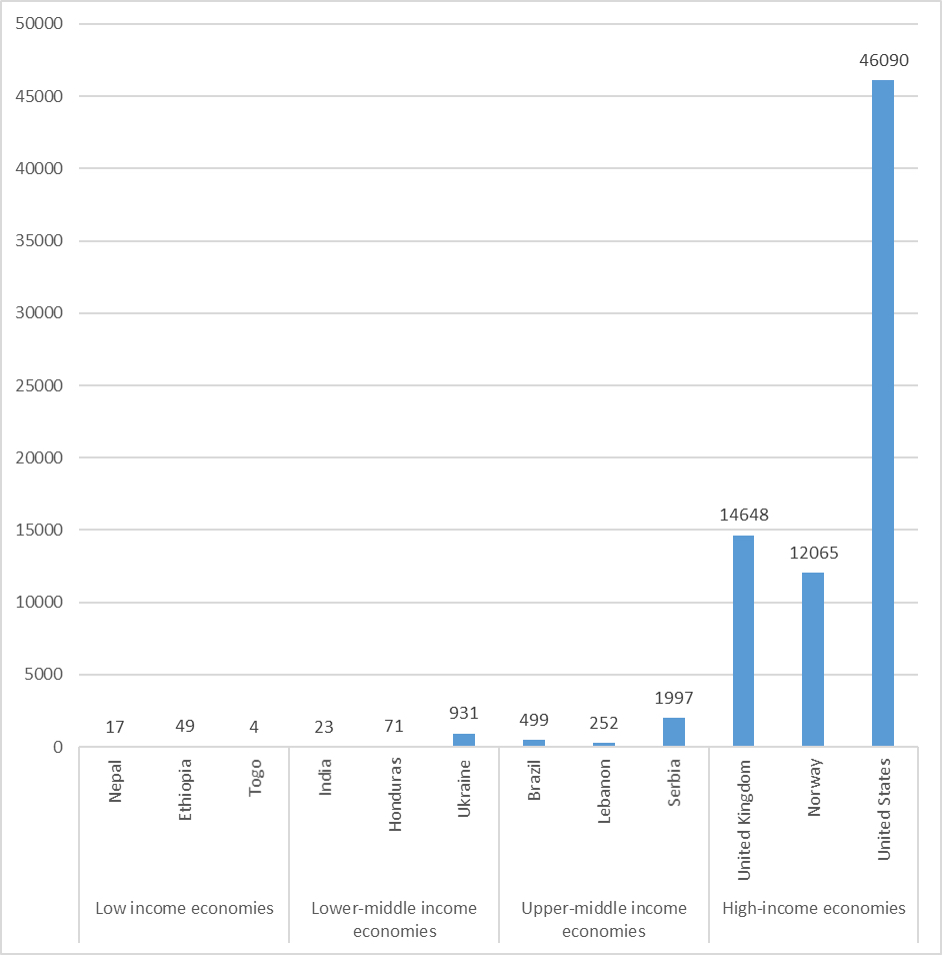
Globally, huge inequities in access to therapeutic opioids are apparent between countries (Figure 4). Whilst the high average consumption in the United States is problematic, the lack of any consumption in some low, lower-middle and upper middle-income countries is alarming. Even in countries where there is some access to therapeutic opioids, availability is inadequate and average consumption far below levels seen in high-income countries. 42,43
Focussing upon availability of opioids for therapeutic use will reduce avoidable suffering globally and decrease illicit demand for opioids for legitimate clinical purposes. Global facilitatory leadership from the INCB is required to re-frame discourse around therapeutic opioids and increase appropriate access around the world, whilst preventing a repetition of the circumstances which have led to a crisis relating to over access in some high income countries.44 In some high use countries where there has not been an explosion of addiction, there are lessons for countries and regions seeking to promote safe and appropriate access to therapeutic opioids for patients.45
After fifty years of regulation by the INCB, appropriate access to opioids around the world remains a global public health crisis. Severe levels of suffering are endured by patients around the world daily, which could be safely reversed with low-cost therapeutic opioids. The INCB must consider urgently how to address the imbalance of attention they provide to improving therapeutic access as a humanitarian emergency. The status quo is a situation where millions suffer seriously each day due to lack of appropriate access to therapeutic opioids for severe pain from acute trauma or surgery.46
Our analysis has strengths and limitations. A key strength of this analysis is the inclusion of all key terms relevant to therapeutic opioids, as defined by MeSH codes within a representative sample of INCB annual reports. Systematic coding of all keywords by two separate researchers, with a third as adjudicator is a robust process. In terms of limitations, we acknowledge that each INCB Annual Report has a specific ‘thematic chapter’ of one specific issue each year. In terms of keywords use, each Report therefore may be biased towards the thematic chapter. The INCB also publishes separate reports with different thematic foci. However, because of separate subject-focussed reports, it is most appropriate to review Annual Reports, for a measured assessment of the overall discourse of the INCB in relation to therapeutic opioids over time. Future research may include a sample of more recent reports to focus specifically on current activity of the INCB as opposed to a historic time-point analysis. This analysis has not sought to address debates regarding opioid-substitution therapy for dependents but notes that an alternative analysis from such a perspective could be fruitful. Finally, in spite of using a systematic approach, there is likely to be some variation in applied codes. However, small variations in coding are unlikely alter composite findings materially.
CONCLUSIONS
In INCB Annual Reports since 1968, prioritisation has been given to the restriction of production, trade and use of controlled substances for illicit use over promoting therapeutic opioids. Urgent international and national action is required to improve methods of accurately estimating population-level needs for therapeutic opioids for all clinical requirements. From there, health systems will have accurate assessments of the extent to which reform is needed to ensure that ‘needs’ and ‘requirements’ for therapeutic opioids become equivalent. Fears of illicit production or use should not limit the prospects of accessing appropriate therapeutic opioids where the majority of the world, today, have no realistic access. Patients the world over and their families deserve better.
Authorship contributions: All authors meet all aspects of ICMJE criteria. Concept; JC, DC, MJ; design MF, JC, DC, MJ: data analysis BF, JC, MJ, DC; data interpretation All; first draft manuscript JC; All authors contributed to manuscript drafts and agreed the final manuscript.
Competing interests: All authors have completed the ICMJE COI form (available upon request from the corresponding author), and declare no conflict of interest.
Funding: This study was funded by the University of Hull and the Academy of Sciences, INSPIRE program. The funders of the study had no role in the study design, data collection, data analysis, data interpretation, or writing of the report. The corresponding author had full access to all data in the study, and all authors had final responsibility for the decision to submit for publication. As INCB reports are available in the public domain, no ethical approval was sought for this study.
Correspondence to:
Dr Joseph D Clark, BA, MA, PhD
Wolfson Palliative Care Research Centre
University of Hull
Hull HU6 7RX
UK
[email protected]