There has been remarkable success in reducing mortality among children less than 5 years old in recent decades resulting in a dramatic 62% reduction in childhood mortality in the time period from 1990 to 2016.1 However, reductions in neonatal mortality have lagged behind, declining only 49% in that same time period.1 Currently, neonatal mortality accounts for 46% of under-five deaths, with 99% of these deaths occurring in low and middle-income countries (LMIC).1 Increasing utilization of healthcare services as a means to improve child health has been a core component of global health and development.2 In recent decades, there has been improvement in the rates of antenatal care, skilled attendance at birth, and postnatal care in low and middle-income countries.3 However, increased healthcare utilization is often not accompanied by high quality of care, limiting the impact on neonatal health outcomes.3
Oxygen therapy, one of the most widely used neonatal care interventions in high-income countries, is an essential part of emergency neonatal care.4 It is used for treatment of many important causes of neonatal morbidity that result in hypoxemia, including respiratory distress syndrome, asphyxia, infection, and other primary lung diseases.5 However, inappropriate use of oxygen therapy in neonates can also lead to serious adverse consequences.6 In the post-World War II era, retinopathy of prematurity was a leading cause of blindness in Europe and North America, with unmonitored oxygen therapy as the major risk factor.7 Evidence suggests that another epidemic of retinopathy of prematurity is occurring due to widespread unmonitored oxygen therapy in premature infants in low and low-middle income countries.8
Developing and implementing global newborn health strategies warrants a broad understanding of the state of neonatal oxygen therapy in low and middle-income countries. In our pragmatic review, we aim to assess and summarize the peer-reviewed literature on the state of neonatal oxygen therapy in low and low-middle income countries between 2007 and 2017, as well as identify key research and programmatic gaps relating to the quality of neonatal oxygen therapy in this environment.
METHODS
Search strategy
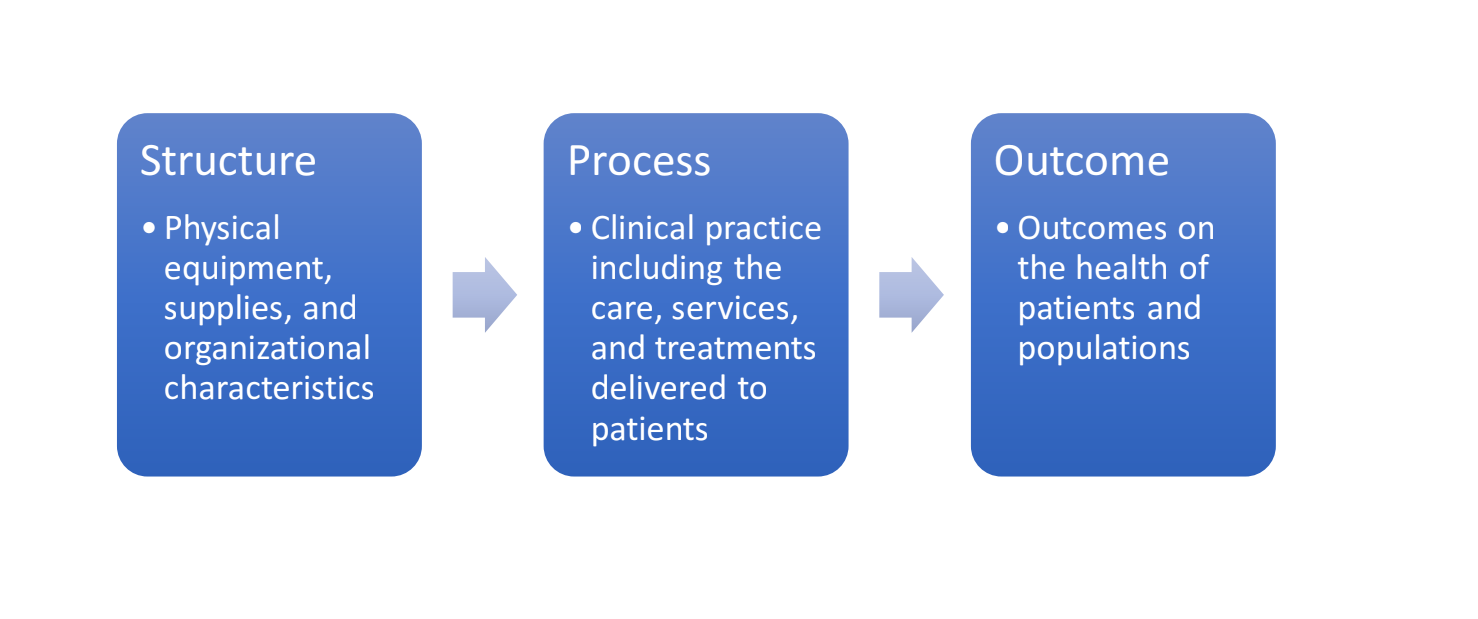
We conducted a literature search in three online databases (Pub Med, EMBASE, CAB Global Health) and amongst USAID’s country-based sampled health facility assessments, known as “service provision assessments.”9 We used the Donabedian model of healthcare quality to guide and organize our review (Figure 1).10 Based on the dimensions of quality described in the Donabedian model, we focused the review on the availability of physical equipment and consumables needed for neonatal oxygen therapy, clinical practices relating to neonatal oxygen therapy, and the outcomes and complications of neonatal oxygen therapy.

To reflect the current state of neonatal oxygen care, we limited our search to publications in the previous 10 years before our search was conducted (2007-2017). We limited the countries included in the search to low-income and low-middle income countries according to the 2016-2017 World Bank country groups. Search terms reflected equipment and supplies needed for oxygen therapy (pulse oximetry, oxygen cylinders, etc.), associated complications (retinopathy of prematurity, bronchopulmonary dysplasia, etc.), other terms that select for neonates (neonate, newborn, etc.), and terms identifying the countries of our search. The search terms used for the search of the PubMed dataset are provided in Figure S1 in the Online Supplementary Document. Articles that provided information on clinical practice and training, physical equipment including consumables such as electricity and oxygen source, and outcomes of oxygen therapy were included. Exclusion criteria were: (a) research on animal rather than human subjects, (b) entries in languages other than English, (c) countries not categorized as low or low-middle income, (d) study not providing information specific to neonates, (e) study not describing the availability or use of physical equipment and materials needed for oxygen therapy, the clinical practice of neonatal oxygen therapy, or the outcomes of neonatal oxygen therapy, (f) publications focused on invasive forms of mechanical ventilation, and (g) full text not available.
Literature search
We identified 474 records from the initial search of the databases and an initial search of the previously described USAID Service Provision Assessments. After removal of the duplicates and reviewing the titles for country relevance (low or low-middle income country), and time period (2007-2017), we selected 132 records. We reviewed abstracts of the selected records to ascertain information on location, time period, and relevance of information for the neonatal age group; 100 publications met the eligibility criteria for review of the full publication. We then reviewed the full text of the selected abstracts to determine whether inclusion criteria were met. Excluded publications were coded according to the reason for exclusion and appropriate data was extracted from the 26 entries that met the inclusion criteria. The extraction process that followed focused on information in the following categories: general study characteristics (title, author, year, location, and study design), physical equipment, clinical practice, clinical outcomes, summary, and bias assessment.
RESULTS
For each of the dimensions of quality described in the Donabedian model (structure or physical equipment, process or clinical practice, and outcomes) we have summarized our results in summary tables (Table 1, Table 2 and Table 3).
A) Physical equipment of neonatal oxygen therapy
For the structural dimension (physical equipment and consumables), we examined five categories of provisions needed for appropriate neonatal oxygen therapy: (a) availability and use of oxygen, mode of oxygen storage, and general supplies needed for oxygen therapy; (b) materials used to modify the oxygen being provided (e.g. oxygen blenders, flow splitter, heaters, humidifiers, and continuous positive airway pressure (CPAP) devices); (c) patient interface with the oxygen (eg. nasal prongs, nasal cannula, nasopharyngeal cannula, oxygen hood, or face mask); (d) equipment used in the monitoring of oxygen therapy (pulse oximeters or multi-parameter monitors); and (e) maintenance and repair of the equipment. The findings of this review on physical equipment used in the provision of neonatal oxygen therapy are summarized in Table 1.
Physical equipment: availability of oxygen and oxygen storage
One Service Provision Assessment and five peer reviewed publications provided information on service readiness and availability of neonate-specific oxygen therapy at health facilities in low and low-middle income countries.11–16 Three of the five publications independently described oxygen concentrators in use at a single referral hospital, Queen Elizabeth Central Hospital in Malawi, over different time periods with Heuvel et al. describing the installation of the oxygen concentrators in 2011 and their use at points during the subsequent three years following installation.11–13
Sa’avu et al. assessed the availability of resources needed for high quality treatment of childhood pneumonia and neonatal illnesses before a quality improvement intervention in five rural district hospitals in Papua New Guinea, and was the only article to provide information about electricity supply, cost, and logistical issues pertaining to neonatal oxygen therapy.16 Oxygen cylinders were used as the source of oxygen by all hospitals and the most commonly cited barriers to oxygen availability were a lack of funding for transport of oxygen as well as problems that occurred in the transport of oxygen such as road closures due to local conflicts and landslides.16
The Service Provision Assessment conducted in 2010 in Kenya surveyed health care facilities that provide care for neonates, including neonatal oxygen therapy.14 Assessors reported that 75% of all hospitals (a definition encompassing district hospitals, provincial hospitals, and referral hospitals) and 37% of all facilities (hospitals, health centers, maternities, clinics, and dispensaries) offering labor and delivery services had an oxygen source available.14
Physical equipment: materials used to modify the oxygen flow, humidity, pressure, or content
Most of the information in the literature involving material used to modify the oxygen administered to neonatal patients was related to continuous positive airway pressure devices (CPAP). Eight publications described some form of continuous positive airway pressure device (bubble CPAP, nasal CPAP, and a variable flow jet CPAP) in use as a part of the description of a related clinical trial or observational study.11,12,17–22 These studies all took place at neonatal intensive care units or referral hospitals with five studies from India, two from the same hospital in Malawi, and one from Egypt.11,12,17–22
Two randomized controlled trials of high-flow nasal cannula utilized equipment to heat and humidify oxygen, but no publications addressed the provision of clean water for such humidifying units.17,20 Three studies provided indication of the installation or use of flow splitters,11,16,20 but Hundalani et al., mentioned that “many district hospitals in Malawi do not have flow splitters that would allow the delivery of < 1 L/min oxygen” in the discussion of their 2015 study.12 Finally, Osman et al., provided the only description of oxygen blenders and flow meters in the reviewed literature.20
Physical equipment: patient interface devices
Nine publications provided information on patient interface devices with six describing studies completed in South Asia, two conducted in Malawi, both at Queen Elizabeth Central Hospital, and one conducted in Egypt; all studies described referral hospitals.11,12,17–23 The most common patient interface was nasal prongs used in conjunction with a CPAP device (three articles representing three hospitals in India, one in Pakistan, one in Egypt, and one in Malawi).11,12,17–20,22
Of the nine publications with information on patient interface devices, only three provided some description of the sizes of nasal prongs available, as neonatal sizes are generally accepted as necessary to administer oxygen to neonates with such an interface. Tagare et al. described the availability of “appropriate sizes” of nasal prongs at a neonatal intensive care unit (NICU) in India and Osman et al. described the availability of five different sizes of nasal prongs at a university hospital in Egypt in the methods section of their respective randomized control trials.20,22 Meanwhile, Heuvel et al. described nasal prongs being available in both infant and neonatal size at Queen Elizabeth Hospital in Malawi in 2011.11
Heuvel et al. also indicated that the binasal prongs were reusable and that the standard protocol was to clean the prongs with soap and water followed by alcohol following each use.11 No other publications addressed nasal cannula, nasal prong, or tubing replacement.
Physical equipment: monitoring equipment
A total of 10 publications reported data on equipment used in the monitoring of oxygen delivery, describing 6 studies conducted in Southern Asia, 3 conducted in Africa, and 1 in Southeast Asia. The publications in Africa were set in a tertiary care hospital and the main referral hospital in Malawi. 11,12,15–17,21,23–26 The publications from South Asia reflected studies conducted at tertiary care hospitals or neonatal intensive care units in India and Pakistan.11,15,17,21,23,26 The only study from Western Pacific Region was conducted in five rural district hospitals in Papua New Guinea.16
Two of the publications reported on situations where pulse oximetry, or other equivalent monitoring device, was unavailable or insufficient. In a 2014 study describing the features of 15 infants with aggressive posterior retinopathy of prematurity who had been referred to an Indian tertiary care hospital from lower level nurseries, Sanghi et al. found that “all infants received unmonitored oxygen for prolonged duration.”25 Sa’avu and co-workers specifically assessed the availability of resources needed for quality care of childhood pneumonia and neonatal illnesses before a quality improvement intervention in five rural district hospitals in Papua New Guinea.16 They found that although all five hospitals had pulse oximeters, they were available only in operating rooms and used by anesthesiologists, and not for sick neonates.16
All other reports describing the use of pulse oximetry were not from publications specifically examining use in the population, but rather from publications evaluating the outcomes of oxygen therapy in selected centers or publications detailing the installation of new oxygen therapy equipment.11,12,15,17,21,23,24,26 All of these publications indicated that pulse oximetry was available in the specified health facility in the course of the evaluation.11,12,15,17,21,23,24,26
Only one publication reported information on neonatal-specific probes or the reuse or replacement of pulse oximetry probes. Sa’avu et al., again reporting on five district hospitals in Papua New Guinea in a study published in 2014, found that none of the hospitals (0/5) had neonatal sensor probes for their pulse oximeters.16
Physical equipment: maintenance and repair feasibility
Sa’avu and co-authors also addressed maintenance of equipment necessary for neonatal oxygen therapy.16 They found that, amongst the five district hospitals in Papua New Guinea, most of the equipment being used before the intervention was donated and therefore, difficult to maintain.16 No other publications addressed the maintenance or repair of equipment necessary for neonatal oxygen therapy.
B) Clinical practice of neonatal oxygen therapy
We explored four issues under the process dimension of the Donabedian framework; (a) the recognition of the need for initiation of oxygen, often accomplished through clinical signs or oxygen saturation (SpO2) monitoring; (b) the fraction of inspired oxygen (FiO2) used; (c) the monitoring of ongoing delivery of oxygen; and (d) the cessation of oxygen therapy (Table 2).
Clinical practice: initiation of oxygen therapy
One study provided information on the initiation of oxygen therapy. Heuvel and colleagues’ study at Queen Elizabeth Central Hospital in Malawi described the usage of a newly installed CPAP machine, consisting of a compressor, oxygen concentrator, water bottle to control the pressure and binasal prongs.11 The study found that in the first seven weeks of use 11 neonates were treated with CPAP therapy, of whom only five met the inclusion criteria.11 Additionally, 20 other neonates met eligibility requirements for the usage of CPAP, but did not receive the therapy due to unavailability of device or clinical error.11 The study also notes that after this initial introductory period the frequency of use declined even further.11
Clinical practice: fraction of inspired oxygen (FiO2)
One study provided information on FiO2 in routine neonatal oxygen therapy.21 Rohit et al., in an observational study of different methods of ventilation at an NICU in India, described a practice of starting FiO2 for nasal CPAP at 0.4 for neonates with respiratory distress receiving nasal CPAP oxygen therapy at the onset of the therapy.21
Clinical practice: monitoring of oxygen therapy
Two publications provided information on goal oxygen saturation (SpO2) range used to guide oxygen therapy in neonates.24,26 Adio et al., in a cohort study that screened premature neonates to determine the incidence and risk factors for the development of retinopathy of prematurity at a teaching hospital in Port Harcourt, Nigeria noted that neonates were treated with oxygen therapy at a goal range of 90-95% SpO2.24 Likewise, Sathar et al., in a cohort study of retinopathy of prematurity development in premature neonates, described a goal SpO2 of 93-95% and indicated that monitoring with pulse oximetry was continuous.26
Clinical practice: cessation of oxygen therapy
No publications provide information on the clinical guidelines or practices leading to the cessation of oxygen therapy in neonates.
C) Outcomes of neonatal oxygen therapy
Most of the recent peer-reviewed literature providing information on the outcomes associated with neonatal oxygen therapy focuses on the development of retinopathy of prematurity and its association to oxygen exposure (Table 3).
Adverse outcomes: retinopathy of prematurity (ROP)
Fourteen publications provided information on the relationship between neonatal oxygen therapy and retinopathy of prematurity, with eleven of those publications describing studies in South Asia, one in Egypt, and another two in Nigeria.7,21,24–36 All of these publications reflected studies conducted at tertiary care hospitals and described neonates who had been given care in their facility.7,21,24–34,36
Eleven out of the fourteen publications described cohort studies that selected a group of neonates with risk factors for retinopathy of prematurity and attempted to describe the prevalence and risk factors for the development of retinopathy of prematurity.21,24,26,27,29–34,36 The selection criteria for the neonates varied from study to study, but generally involved gestational age and weight criteria for screening, and then included other neonates who met other risk factors for retinopathy of prematurity.21,24,26,27,29–34,36 Clinical information on the monitoring of oxygen therapy in neonates was not provided in nine out of the eleven publications, while Sathar et al. and Adio et al. each described continuous monitoring of SpO2 on a pulse oximeter with a target SpO2 under 95%.21,24,26,27,29–34,36 Of these eleven publications, four found oxygen therapy to be significantly associated with retinopathy of prematurity, and six found oxygen therapy to be a risk factor for the development of retinopathy of prematurity.21,24,26,27,29,31–34,36 The eleventh study found oxygen therapy to be associated with retinopathy of prematurity, P=0.11, but not significantly so.30 The incidence of retinopathy of prematurity ranged from 11.9% to 25% in South Asia, 15% and 47.2% in the two publications that described hospitals in Nigeria, and 19.2% in the study from Egypt.21,24,26,27,29–34,36 Three publications, all studies conducted in India, calculated odds ratios for the development of retinopathy of prematurity in the presence of neonatal oxygen therapy, and found odds ratios of 1.89 (confidence interval CI=1.06-3.39), Chaudhari et al., 2.4 (CI=1.1-5.4), P.S. Kumar, M.J*. et al*., and 2.042 (CI=1.221-3.416), Sathar et al.23,26,31
The objective of the other three publications, including two case series and one case control study, was to describe the outcomes or characteristics of the neonates who had already developed the disease.7,25,28 In contrast to the cohort studies above, these studies described children who had been treated at an outside hospital and then were referred to their tertiary care facility after having developed retinopathy of prematurity.7,25,28 All three of the publications indicated that all children who developed retinopathy of prematurity had received unmonitored oxygen therapy at the original treating hospital, and postulated that oxygen therapy is at least a contributing factor in the development of retinopathy of prematurity in the neonates studied.7,25,28
DISCUSSION
Maintenance and indirect costs associated with the procurement of oxygen may constitute significant barriers to oxygen supply.16 When oxygen is available in facilities, neonates with potential to benefit might not receive therapy in some facilities because of limited equipment, shortage of staff, and unfamiliarity with the technology.11 When neonates receive oxygen therapy, the most common regulating or conditioning equipment described in the literature is CPAP and the patient interface used is variable, but is often some form of nasal prongs.11,12,17–23 While pulse oximeters are used for monitoring of neonatal oxygen therapy in many healthcare facilities, there are examples within the published literature of hospitals delivering neonatal oxygen therapy without necessary monitoring equipment.11,12,15–17,21,23–26 Oxygen blenders, which are necessary to titrate the fraction of inspired oxygen (FiO2) and by extension the patient’s oxygen saturation (SpO2), were only described briefly in one study.20
There is a paucity of data on effectiveness of neonatal oxygen therapy in LMICs as currently practiced, as well as important side effects such as bronchopulmonary dysplasia. However, some findings were present in the literature including the suggestion that the usage of a bCPAP device with oxygen as opposed to oxygen therapy through a standard flow nasal cannula or nasal prong in the treatment of neonates with respiratory distress may significantly increase survival for affected neonates.13 Additionally, oxygen therapy was shown by many publications to be associated with development of retinopathy of prematurity and its prevalence among low birth weight and early gestational age neonates and other neonates with risk factors may range from 11.9-47.2%.21,24,26,27,29–34,36
Our findings reinforce the conclusions of Graham et al. that programmatic initiatives for improving oxygen delivery require multi-level and multi-disciplinary interventions addressing all dimensions of oxygen therapy quality.37 A specific issue that is deserving of attention is the availability of monitoring equipment appropriate for neonates. Pulse oximeters available in the facility might not be useful in neonatal care if the probe size needed for neonates is not provided.16 Additionally, the need for constant SpO2 monitoring, in order to avoid dangerous spikes in blood oxygen concentrations, as well as the possibility of the development of hypoxia induced by nasal obstruction places a high demand on clinical personnel administering the therapy. Once the right equipment is in place, clear guidelines are needed to direct the clinical application of neonatal oxygen therapy and quality improvement strategies are needed to ensure consistent application of the guideline. An issue not found in this review, though observed in health facilities by multiple co-authors of this paper, is a system of pay-as-you-go access to oxygen therapy for children in low and middle-income countries. Out-of-pocket payment by families, coupled with the fact that oxygen therapy is often relatively expensive in such settings, poses a further barrier to providing quality oxygen therapy in neonates for an adequate duration and creates an inequitable distribution of potentially life-saving therapy.
It appears that rates of retinopathy of prematurity among neonates of matched gestational age in low and low middle income countries are markedly higher than the incidence rates reported in high income countries.26,27,36,38,39 While this difference may reflect the unmonitored use of oxygen therapy or variable practice with respect to target saturations, it also raises a question as to whether infants in low and middle-income countries might be more vulnerable to toxicities associated with exposure to therapeutic oxygen. Co-morbidities present in middle and low-income countries including malnutrition and increased risk of infection may potentiate risks of oxygen exposure, raising further concerns that vulnerable organ systems, including the cardiovascular system, lungs and brain, might also be at greater risk of toxicity with oxygen therapy.
This review also highlights a number of gaps in the literature and opportunities for further study (Table 4), including the paucity of systematic data that can guide policy, global programming initiatives, and accountability. Most of the publications reviewed did not provide direct estimates across health systems of neonatal oxygen therapy equipment or related clinical practice. The one study that does, the 2010 Kenyan Service Provision Assessment, provides an estimate of the prevalence of neonatal oxygen therapy within the country, but the loose criteria of having either an oxygen concentrator, oxygen cylinder, or oxygen distribution system at the time of assessment does not go far enough to assess if all of the necessary equipment is available for the proper and safe provision of oxygen therapy at these facilities.14 Surprisingly, of the USAID Service Provision Assessment reports reviewed, Kenya was the only report that provided information on neonatal-specific indicators. Future reports would benefit from standard neonatal-specific assessments and tabulations given that neonatal mortality represents a growing fraction of under-five deaths as a whole. For oxygen therapy specifically a reasonable assessment of a facility’s readiness to administer neonatal oxygen therapy might include questions on: (a) availability of a source of oxygen (i.e. oxygen cylinders, oxygen concentrators, etc.), (b) availability of patient monitoring equipment during oxygen therapy including neonatal specific probe availability if using a pulse oximeter and a reported frequency of monitoring during therapy, and (c) questions on the availability of oxygen blenders in order to be able to titrate the amount of oxygen given.
Another gap is the paucity of information about oxygen blenders in the literature, with only one study mentioning their availability. While, traditionally, oxygen blenders have been cost-prohibitive in resource-limited settings, recent technological advances in the creation of low-cost oxygen blenders may make them more widely available and published literature on their availability and use will likely be important going forward.40 Additionally, there are no reports of the specific barriers faced by clinicians in appropriately initiating or ceasing neonatal oxygen therapy. Finally, and of significance, is the paucity of reports of system-wide assessments of availability and usage of pulse oximeters to monitor neonatal oxygen therapy and the multiple indications that facilities are currently giving oxygen without pulse oximeter monitoring. The ethical commitment to ‘do no harm’ and the well-established side effects of unmonitored oxygen therapy make large-scale monitoring and evaluation of use of pulse oximeters, oxygen blenders, and other important equipment a priority.
There were several limitations to our review. First, we conducted our literature search only in English and, therefore, have excluded other neonatal oxygen therapy reports published in Spanish, French, Arabic, and other languages. Second, many of the publications in this review were not focused on the review objectives, and only provided incidental information on the quality of neonatal oxygen therapy. Third, the health care facilities that are represented in this paper may not be a representative sample to provide a picture of the quality of neonatal oxygen therapy in low and low-middle income countries. Published literature inherently reflects more advanced care as authors are more likely to be in academic settings, and therefore our review would be more likely to under-report the burden of unmonitored or inappropriate oxygen use. This is particularly relevant with respect to the generalizability of outcomes of oxygen therapy. Most publications that described retinopathy of prematurity incidence in neonates treated at tertiary care facilities were assumed to have received optimal clinical practice in the provision of oxygen therapy,21,24,27,29–34,36 while other publications that described the outcomes of neonates treated at health care facilities of a lower tier that were later referred to a tertiary care facility often described unmonitored oxygen therapy as the primary driver in the development of retinopathy of prematurity.7,25,28 Fourth, the scope of our review did not include other important resources such as the WHO Service Availability and Readiness Assessments (SARA) or country-level Emergency Obstetric and Newborn Care (EmONC) assessments.
CONCLUSIONS
Maintenance and indirect costs associated with the procurement of oxygen may constitute barriers to oxygen supply.16 When neonates receive oxygen therapy, the most common regulating or conditioning equipment described in the literature is continuous positive airway pressure devices, and the patient interface used is variable, but is often some form of nasal prongs.11,12,17–22 Pulse oximeters used for monitoring of oxygen therapy are available in healthcare facilities, but there is very little known about the frequency of that monitoring and there are indications that hospitals deliver neonatal oxygen therapy without necessary monitoring equipment at all.11,12,15–17,21,23–26 Oxygen therapy is associated with the development of retinopathy of prematurity and its prevalence among low birth weight and early gestational age neonates and other neonates with risk factors may range from 11.9-47.2%,21,24,26,27,29–34,36 which appears to be higher than rates in neonates of similar gestational age being treated in high-income countries.26,27,36,38,39 Quality improvement initiatives to create standardized guidelines for the appropriate and safe use of neonatal oxygen therapy and address adherence to those guidelines may reduce the burden of associated morbidity and potentially save the lives of neonates in low and low-middle income countries.
Disclaimer: The views and opinions expressed in this paper are those of the authors and not necessarily the views and opinions of the United States Agency for International Development.
Funding: No specific funding was required to perform this study.
Authorship contributions: Conceived the study: PKR. Developed framework and organized the search: PKR, MO, JZ. Wrote the first draft of the manuscript: JZ. Wrote and approved the paper: All authors.
Competing interests: The authors completed the Unified Competing Interest form at www.icmje.org/coi_disclosure.pdf (available upon request from the corresponding author), and declare no conflicts of interest.
Correspondence to:
Jon Zelasko BA, MD candidate 2020
Jacobs School of Medicine And Biomedical Sciences
University at Buffalo
955 Main Street
Buffalo, New York 14203
United States of America
[email protected]