The largest religious affiliation in South Africa1, the Christian Church has been involved in the HIV/AIDS epidemic since its identification in the 1980’s. The Church’s stand on sexuality (ie, within the context of marriage only), and the traditional relational practices (eg, having multiple partners outside of legal marriage) have all led to a complex relationship with HIV/AIDS.1,2 The reactions of various Church groups in South Africa has varied from silently ignoring the disease (more common reaction) to openly condemning those who have been ‘sexually immoral’ and need to ‘repent’ of their sins.3–5 This condemnation resulted in strong stigma against the disease and its victims, pushing Christian South Africans to not want to know their HIV status thereby delaying treatment, and to not disclose their status when they do find out for fear of judgment and rejection.4 In the end, disclosing HIV status may lead to rejection and criticism from the religious community, while keeping silent about positive results may undermine a person’s identity and ability to cope with the disease.4
Despite the existing stigma, the importance of the religious or faith community in the lives of persons living with HIV/AIDS (PLWHA) has been demonstrated in many sub-Saharan African regions. HIV infected Africans living in England6 have been found to attribute great importance to their faith in the management of daily life; at the same time, they viewed the Church as a threatening space marked by lack of confidentiality, and a site for the generation of stigma.6 Among HIV infected Africans in England7 and in Malawi 8, personal level of religiosity, that is their faith and belief9, has also been found to influence the type of treatment sought, with PLWHA often looking to religious leaders for healing rather than modern medicine.10 Studies from Sub-Saharan Africa8,11,12 have found that attendance in faith healing congregations was associated with lower levels of generalized worry about AIDS and neglect of modern medical treatment for HIV. In South Africa, a study of complementary medicine in KwaZulu-Natal found that spiritual practices and prayer were common practice (77.6% of sample) for stress relief among HIV infected individuals.13 A study in the US has shown that religiousness/spirituality among HIV infected individuals was associated with slower disease progression when it complements modern medicine.14 With HIV becoming more of a chronic condition, more data on the role of religion is needed to better understand the needs of PLWHA, especially in South Africa where the Church has historically played an important role in the lives of the Black population.
Indeed, the Church in South Africa continues to have a strong social role in communities, making it an important stakeholder in the fight against the HIV/AIDS epidemic.3 Thus far, the activity of the Church in South Africa in fighting the HIV/AIDS pandemic has been less than impressive and “best described as a series of notable exceptions against a backdrop of silence”.3 Although improvement is slow, some recent religious organizations’ efforts have been perceived to dissuade related stigmas by increasing openness and leadership. A specific example of a successful intervention is the Khayelitsha Fikelela program founded in 2001 in the Anglican Church, with the slogan: “This church is HIV/AIDS friendly”.15 Its success led to the Anglican Church mandating and financially supporting the program in their Churches in South Africa.15 In 2003, the South African Church Leaders’ Association (SACLA) designated HIV/AIDS a priority, alongside poverty. Since, several denominations have made official efforts, albeit fragmented, to address HIV/AIDS, with varying degrees of success.15 Most of these Church-based efforts addressed HIV/AIDS-related stigma in primary and secondary prevention, raising awareness about HIV/AIDS and encouraging testing and screening. Little effort has focused on tertiary level interventions, caring for PLWHA. Despite the decrease in HIV incidence (1.90 in 2002 to 0.91 in 2017), the prevalence in the country remains high (12.6%), with the majority of the estimated 7 million (2017 estimate) of PLWHA being Black. The black population in South Africa holds the highest rate of HIV at 13% compared with 0.3% for Whites.16,17
To better inform faith-based interventions, it is therefore important to explore Church leaders’ perceptions of the role the Church can play in providing spiritual guidance and social support to PLWHA in Black communities. This study explores Christian religious leaders’ perceptions of PLWHA, current support provided to them, and the role of religious institutions in addressing the spiritual, health and social needs of PLWHA in the Black Townships of Soweto.
METHODS
We used a convergent parallel mixed-method18 cross-sectional study design, conducting interviews and surveys sequentially at one visit, and analysing results separately prior to incorporating both qualitative and quantitative data for a merged interpretation of results. Specifically, we used an exploratory approach for in-depth understanding of religious leaders’ perceptions through qualitative methods, while obtaining additional information through quantitative questions. The survey was administered in order to provide descriptive information about the leaders, assess their stigma, and obtain specific details about their perceived needs in the area of HIV/AIDS services. Social desirability may be a factor that often comes into play when interviewing community leaders, whether in politics or religion. We selected a stigma scale to permit anonymous responses, increasing chances of accuracy in reporting and allowing for comparison with qualitative responses.
Setting
The study was conducted in Soweto, a peri-urban township 15 kilometres (km) to the southwest of Johannesburg, South Africa. Soweto – an acronym for South Western Townships - is divided into several townships, and was created around the 1930s as a black settlement area during apartheid. Soweto spans an area of 63 km2 and the population is reported to be approximately 1.1 million, but is variably estimated to be larger, at between 2.5 - 3 million people, almost all being Black.17
Participants
A total of 45 religious leaders (see Table 1) completed a self-administered survey on demographics, their religious institution’s characteristics and beliefs about PLWHA, services and support offered of benefit to PLWHA, and barriers to providing additional services and support targeting PLWHA. Of the 45 leaders invited to participate in both the completion of a survey and a group discussion or an individual interview, 26 agreed to participate in in-depth interviews to further learn about their current efforts towards serving PLWHA in their respective congregations, and obtain their perceptions and experiences related to HIV and PLWHA. The original aim was to interview approximately 50% of survey participants or until data saturation18 was reached. A total of 26 survey respondents (58% of the sample) participated in group or individual interviews.
Data collection
Religious leaders were invited by telephone to participate between June 2014 and August 2016. An adult HIV prevention Community Advisory Board (CAB) assisted with facilitating meetings among religious leaders in Soweto. Religious leaders were to be of any branch of the Christian religion and serve members of the Soweto Townships. An initial focus group discussion with 6 religious leaders who assisted with the recruitment of others to complete a survey and a select few to participate in interviews. Religious leaders approached for interviews were asked to complete the 15 minute self-administered pencil-and-paper survey in English prior to the discussion. Written consent was obtained for all participants prior to conducting study procedures. All efforts were taken to ensure participant confidentiality. Participants received 100ZAR (approximately US$7) reimbursement for their time and transportation.
Of the approximately 30 approached, 26 agreed to be interviewed. Based on their preference and availability, religious leaders were either interviewed individually (n=6), in a small group of 2 to 3 (n=9) or in a larger focus group (n=11). The location of the interviews were based on participant preference (Church building, community centre or a private training room at a health centre). An additional 19 were approached to complete the survey only. Individual, small group and focus group interviews were conducted by a trained researcher fluent in the local languages, lasted 60 to 75 minutes and were audio recorded (with written participant consent) for later transcription. Interviews and transcriptions were completed by the same researcher for consistency, and coding was developed and verified by 3 researchers of Muslim and Christian religions, to reduce bias. Codes, themes and categories were reviewed and discussed until agreement was reached.
Measures
Demographic characteristics for religious leaders and Church community
The survey assessed demographic information and HIV stigma. The demographic questions included: age, race, gender, marital status, education level, number of years in the ministry, and congregation information (size, general demographic).
HIV-related stigma
The HIV-related stigma scale, developed by Kalichman SC, et al.19 for use in South Africa, consisted of 9 items assessing AIDS-related stigma towards PLWHA. The scale includes responses to statement such as: people who have AIDS are dirty, people who have AIDS are cursed, people who have HIV should be isolated, people who have AIDS should not be allowed to work, etc. The responses are dichotomous: 0=Disagree and 1=Agree. The total score was obtained by summing all the items and a median score of >1 was used as a cut-off. Higher scores indicated greater stigma (α=0.79).
Individual and group interviews began with the scenario method20 to dispel potential interviewer biases, prior to delving into the specific questions. The scenario method is used to elicit reactions and information about specific types of cases without putting any particular person or group (in this case, religious leaders and PLWHA from their congregations) at risk of being exposed or embarrassed about holding certain opinions. The religious leaders were given 3 specific cases and asked to describe the ‘normal’ reactions to such scenarios1: a married woman who contracted HIV as a result of her husband’s unfaithfulness2; a male leader in the Church (to explore potential differences in reactions to Church leaders vs. members) who contracted HIV through homosexual activities; and3 an unmarried woman who contracted HIV from a partner. Follow-up questions were posed based on the reactions towards the individuals in the scenarios, differentiating between the contexts of the Church specifically and the religious community in general. Final questions focused on exploring their perceptions of the role of the Church in the lives of PLWHA.
Statistical methods
The age of participants was stratified into two groups: 22-45 and 46-79 years. Frequencies were determined for categorical variables stratified by age-group. Reliability of the HIV-stigma scale was ascertained using the Cronbach Alpha test.
RESULTS
Characteristics of religious leaders and their Church community
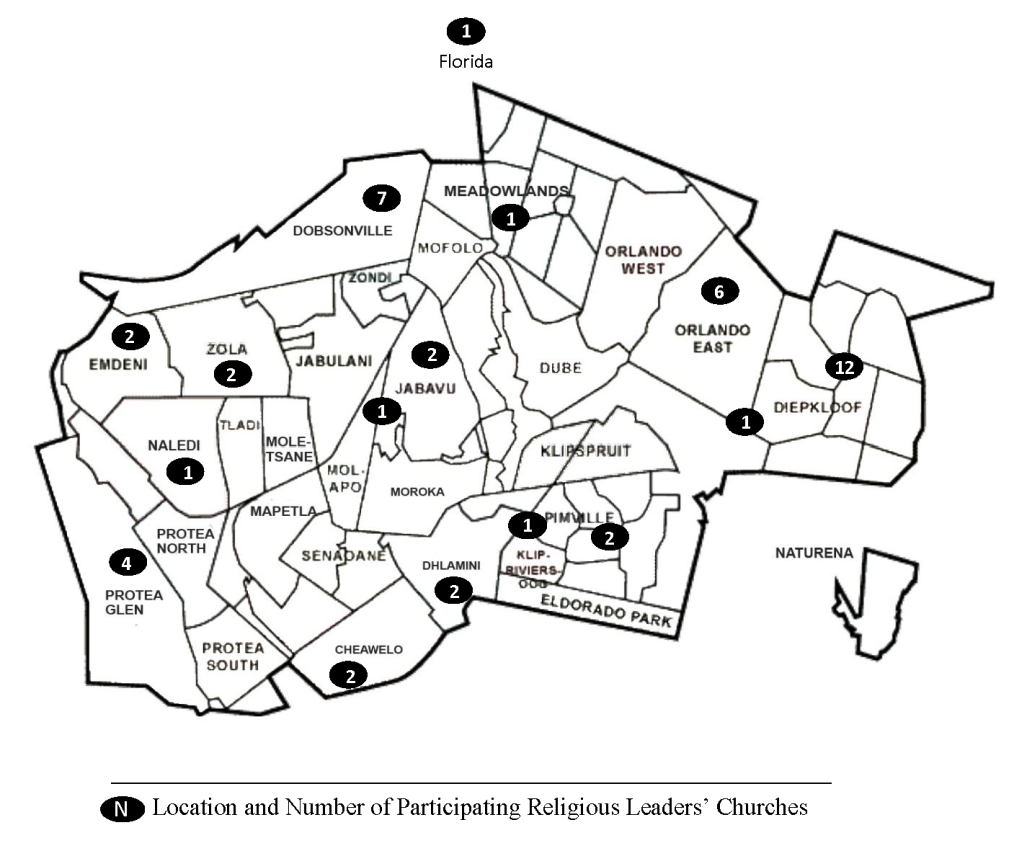
A total of 45 Black religious leaders responded to the survey, with an approximate 90% recruitment rate, and 26 of the 30 approached agreeing to be interviewed individually or in a group discussion. All but one participant had Churches located throughout Soweto, however all reported serving Blacks communities from the Soweto Townships (Figure 1). The sample was mainly male (87%, n=39); the majority of leaders (62%, n=28) were married and had children (78%, n=35), with 66% (n=23) having 2 or more children, and almost all (91%, n=41) completed a minimum of high school education. Most reported their role as Pastor/ Reverend/ Priest (53%, n=24) or Elder/ Deacon (24%, n=11). Two identified as Evangelist, one Health Ministry Leader and five as “Other” (eg, Music Minister, Youth Minister) (Table 1).

Of the religious leaders surveyed, about half (n=26) were from various Christian denominations, including Evangelical, Methodist, Pentecostal, Anglican, Catholic, and Episcopal. The other half (n=24) classified their Church as “other” (eg, Christian, Church of the Later-day Saints, Seventh Day Adventists, Pentecostal). Again, about half reported having approximately less than 250 members (n=23), and having young adults as the predominant age group of the congregation (n=26) (Table 2).
HIV/AIDS and the Church
Almost half of religious leaders reported that HIV/AIDS was of great concern to the Church (49%, n=22) (Table 3). In the survey, all (100%, n=45) of the religious leaders reported that PLWHA would feel welcomed in their religious community. The leaders reported noting fears of HIV/AIDS among their members, including concerns that HIV infected individuals may spread the disease, or that they are immoral people. Overall HIV/AIDS-related stigma scores indicated high levels of stigma (80%, n=36), the behavioural manifestation of self or societal disapproval of PLWHA in the religious community (Table 3).
When asked in the survey about having specific HIV/AIDS related ministries, most (n=20) of religious leaders reported needing help from outside organisations, and having limited financial and educational resources. Many were unsure how to help PLWHA, were cautious in speaking about HIV/AIDS or working with PLWHA due to lack of experience. Another important struggle for several was the duty to respect the principles of the Church while still showing support to PLWHA. A few individuals felt unsure about what activities/ resources would be most helpful, did not see a need in the community for a HIV/AIDS ministry, or did not think having an HIV/AIDS ministry would be well-accepted by the Church community (Table 4).
In interviews, leaders expressed the desire to have: a health, clinic or hospital ministry so they could reach out to PLWHA where they are; more ongoing HIV/AIDS education (rather than the one annual AIDS day campaign); and training on HIV/AIDS education and how to reduce and eliminate stigma. Analysis of individual and group interviews did not reveal any differences in responses and themes.
Perceptions of HIV/AIDS
Most religious leaders stated that HIV was a manageable disease, with some referring to it as a “chronic disease just like diabetes and high blood pressure.” They stressed the importance of encouraging PLWHA to take Antiretroviral (ARV) medication should they need to, and adhering to the treatment regimen: “We need to teach people that through medicine God is still healing”. Nutrition was an aspect that was raised and discussed several times by many participants. Religious leaders stressed that good nutrition was crucial to those living with HIV/AIDS and must accompany medical treatment, and that poor nutrition led to difficulties adhering to treatment. Other primary challenges to adherence to medication reported were inadequate social support, and the inability to travel to clinics – which for many patients were far from their homes – to obtain their medication.
Perception of Persons Living with HIV/AIDS
In all scenarios given and in individual and group interviews, the mode of contracting HIV was the first concern of all religious leaders: “And also it depends on how they contracted the disease. And so the leader will deal with it on condition of how they contracted the disease, but it will be as confidential as it could be.” Was the person married? Married with children? Was the infection a result of infidelity? Was the person in question infected before or after they were married? Other questions were posed in response to concerns raised by religious leaders. Determining whether the infection occurred as a result of improper, sinful behaviour (homosexual activity, sex outside the bounds of marriage) or through someone else’s act (rape, unfaithful spouse, an infected mother) was crucial to the first steps towards reconciliation with the Church and/or religion.
“From the church point of view, it will depend if he’s sexually active with the girlfriend. Did he contract the disease through transgressing the laws of God?”
“For instance, it says here if infection has resulted from transgressing God’s laws, the church advocates the example of the Lord, who condemned the sin yet loved the sinner and encouraged repentance. So it will depend.”
They spoke of the body as the temple of God, necessitating a confession of sin and forgiveness of self and/or others. For individuals in position of leadership within the Church, HIV infection resulting from improper sex (homosexual, adulterous, premarital) required an immediate removal from responsibility followed by a compulsory disciplinary period, and a restoration to leadership or responsibility within the Church. Specifics varied by Church, however all participants were in agreement.
The overarching theme was to “love the sinner and hate the sin.” The end result was to help PLWHA first reconcile with their religion and renounce any inappropriate behaviours. As one Pastor explained: “So I think when people understand the doctrine then their behaviour changes”. For PLWHA who were considered victims, forgiving the responsible party was the first step to rid the person of hate and anger as they learn to live with the consequences of someone else’s acts. However: "We don’t undermine [sin]. But on the other hand, the most outstanding thing is God’s love for them, and them knowing that there is life after HIV [diagnosis]."
Stigma
Lack of knowledge and misconceptions about HIV and its modes of transmission are persistent in the communities of the leaders interviewed. Leaders reported that many in the religious community continue to view HIV as a curse, a death sentence or a form of punishment by God for their behaviour. These behaviours include open judgement, criticism, disdain and rejection of PLWHA in the context of the religious community.
"You know, in the Church it’s difficult to know if someone has HIV, because if that individual doesn’t go around telling people, then we will not know."
To combat stigma in their congregations, religious leaders reported actively encouraging more people to disclose their status to the Church and their families, not only so they may receive targeted support but also to motivate others to disclose and ask for help.
The roles and responsibilities of the Church and its leaders
Based on survey and interview data, leaders consider themselves to be mediators between PLWHA and their partner, family and religious community. For example, a religious leader explained: “if the person then decides whether to tell the family,.. the minister can even assist the family, so that they can feel that it is not a curse.”
The desires of the religious leaders was to make the Church a safe space for disclosure, to offer assistance in terms of referrals for health or social services or other resources in the Church. For example, they could help PLWHA to get employment by connecting them to congregation members working in the same fields.
Secondly, religious leaders saw it as their responsibility to be preachers of condom use, abstinence and faithfulness to partners. Thirdly, they saw themselves as restorers of faith by helping PLWHA address the behaviours that led to the HIV diagnosis: “We agree that we fall from grace…once or twice or even many times…But we just have to keep on restoring it”.
Leaders interviewed provided details about various resources the Churches have that can benefit PLWHA. Prayer support, Church counselling and feeding programs were the primary resources offered PLWHA.
"First of all, just show a lot of compassion, and expression of support. And make the person aware that as a church leader, I’m there for them, to offer any help whatsoever, that we are in a position to assist. And, uh, obviously as well as a church leader, we’ll need to familiarise ourself [with HIV/AIDS] so that we can be able to help.
“Members should reach out with kindness and comfort to the afflicted, ministering to their needs and helping them find solutions to their problems.”
Other resources mentioned included Church support groups, Church-based HIV/AIDS programmes, Church produced materials on HIV related topics such as homosexuality, dating as a Christian, living with HIV, etc., and humanitarian assistance based on the donations by congregation members. For further HIV testing, counselling or spiritual help needed, religious leaders would refer to health care professionals or other religious leaders.
“At the end of the day they’re still a person, and in the church we regard them as a child of God regardless of where they are, and so I feel like that is one of the most important things, because the moment you start labelling them or ill-treating them, or not making it confidential then they become, you know, isolated or feel like they’re being labelled to a certain degree. So, in as much as we can, we counsel and advise and encourage.”
DISCUSSION
In our study, religious leaders confirmed the need for their involvement and leadership in continuing to provide communities with accurate information on HIV/AIDS as a disease, reduce related stigma, support spiritual reconciliation, and increases services specific to PLWHA. Despite decades of HIV/AIDS campaigns in South Africa, Soweto residents continue to see HIV/AIDS through religious lenses, believing it to be a punishment for sinful behaviour or other spiritual causes such as curses. Similar beliefs are persisting in many other Black communities in Africa. In Tanzania21 and Zimbabwe22, for example, sexual behaviours that lead to HIV infection have been viewed as “reckless” and “immoral,” further promoting blaming attitudes and “othering”21-23 of PLWHA. Additionally, same sex marriage is legal in South Africa, yet homosexuality continues to be deemed improper. This further indicates the influence of religious beliefs that often co-exist with or even trump scientific facts and laws.
These beliefs about HIV fuel stigma towards the disease and those living with it. PLWHA live with constant fear of judgement from their religious community in Soweto as well as in others across the world. This leads to fear of disclosure of their status and renders difficult religious leaders’ efforts to address the specific needs of PLWHA in their congregations, as described by those interviewed in this study.
The scenario method allowed for discussion of stigma among Church leaders and religious communities without participants having to reveal their own beliefs about PLWHA. However, interpretation of the apparent high level of acceptance of PLWHA in this group might be somewhat more negative in reality since none would want to be seen or have their community seen as judgemental or unforgiving. In studies in other similar communities, PLWHA have described their Church leaders’ open rejection and criticism of HIV infected individuals.21–26 Additionally, the stigma scale demonstrated a high rate of stigma among the respondents. Therefore, in the qualitative interviews there may have been an element of performance theory, which posits that leaders often openly speak publicly in a manner that they believe is expected of them rather than what they truly believe as individuals.27,28 Regardless, leaders interviewed did recognize the judgment and stigma existing in their Church communities. They reported their desire to address HIV/AIDS openly in their Churches but recognized that they are reluctant to do so and need the appropriate assistance and training on how to approach the topic with their congregation. This need for training has been concluded in other studies, all calling for more formal training in how to address taboo subjects of sexuality and HIV/AIDS in religious contexts.29,30
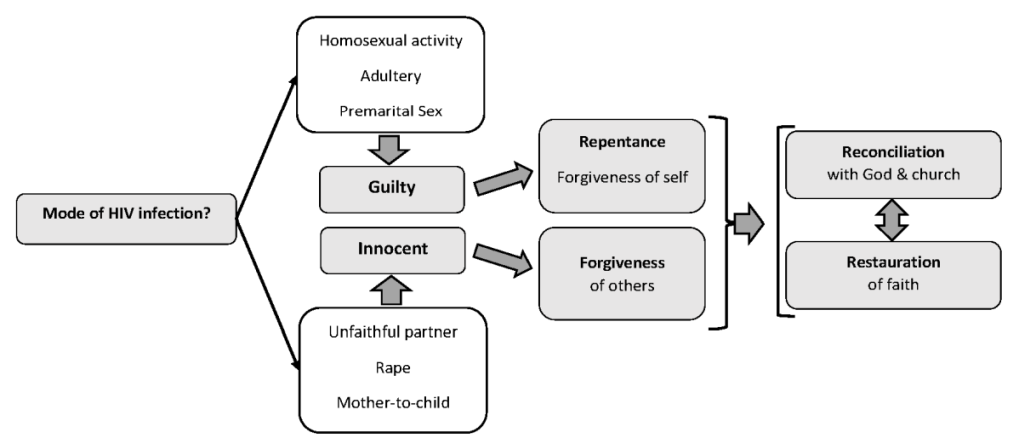
When presented with a case of a member of the parish/congregation/community with a positive HIV diagnosis, religious leaders interviewed and surveyed described the process clearly. As displayed in Figure 2, prior to helping PLWHA, they first must understand the mode of transmission in order to mentor and guide them through the appropriate process. Should they have contracted HIV through “sinful behaviour” such as sex outside the bounds of marriage (adultery, pre-marital sex) or while doing drugs, they would need to first repent and then ask God for forgiveness: "If he contracted the disease through disobeying God’s commandments in this regard, having sex before marriage, then the repentance process will have to follow." They mention an element of self-imposed guilt that the PLWHA must deal with and forgive themselves as well. This would lead to reconciliation with God and self, and bring about spiritual restoration.

“Part of restitution or restoration of things - unfortunately with sexual intercourse you cannot restore but you can amend and move forward so that you don’t repeat the same act again in a manner of transgression. So, one of the things which he may need to do is to open up to his girlfriend, to be honest with her, and have a way forward that, you know, as he’s doing this change of heart and change of mind, that he will then need to abstain.”
“[Homosexual] behaviour violates the commandments of God. It’s contrary to the purposes of human sexuality, and deprives people of the blessings that can be found in family life and in the same ordinances of the Gospel. Those who persist in such behaviour or who influence others to do so are subject to Church discipline. Homosexual behaviour can be forgiven through sincere repentance.”
In the event the PLWHA was “innocent” and contracted the virus through another’s poor behaviour, such as rape, an unfaithful spouse, or transmission from mother to child, then the process of restoring their faith requires the PLWHA to forgive the person(s) who infected them. Dealing with the anger and the hurt through forgiveness would be essential to the restoration of their faith. In both situations, the participating religious leaders saw themselves as helping PLWHA go through these processes.
In addition to assisting the individual spiritually, the leaders also saw themselves as mediators between the PLWHA and their spouses, families and communities, helping them acknowledge the infection of their loved one and work through the acceptance process. Finally, the leaders saw themselves as “Preachers” not only in the religious sense, but in the context of HIV/AIDS, providing accurate information about the condition, preaching tolerance, and reducing the fear of HIV, PLWHA and related stigma.
The leaders in our study reported not knowing many PLWHA in their congregation, but wanted to encourage disclosure as a step towards reducing stigma and identifying those in need of spiritual help and specific HIV/AIDS related services and support. However, PLWHA are often reluctant to reveal their status due to the fear of rejection and judgement from their families and/or Church community.2,4,6 Therefore, it would be important to implement appropriate interventions to reduce stigma in the community prior to expecting PLWHA to disclose their status. A few Churches in South Africa have been actively engaged with the community to increase awareness and education, to reduce stigma, and to encourage care and compassion for PLWHA.3 The Anglican Church in Western Cape, with the activism of Archbishop Desmond Tutu, has been recognized to be at the forefront of the South African Churches’ effort to openly and positively address HIV and related issues within the community.3 Evidenced-based interventions for reducing stigma within the religious community toward PLWHA and caring for PLWHA are lacking and coordination of these Church-based efforts has remained fragmented throughout the country.3 Church-based interventions in other countries with high HIV rates have had to address similar issues pertaining to stigma related to the issues of perceived sexual behaviours.21–26,29–35 In the United States where African Americans bear the burden of the HIV/AIDS epidemic (Accounting for 44% of all new infections as well a 44 percent of PLWHA, while representing only 12% or the total population)35,36, the fight to reduce stigma towards PLWHA continues.37,38
Four broad requirements of an effective intervention are identified across the breadth of HIV literature: 1) creation of a safe and supportive environment that fosters togetherness29,39, 2) attention and encouragement at personal and community levels25,29,39–41 3) stigma reduction and encouraged status disclosure16,26, and 4) resources for treatment and coping.3 These are in line with the religious leaders in our study’s desire to serve as mediators between PLWHA and their families and communities, provide spiritual, social and material support, improve accurate knowledge about the disease, and reduce related stigma. Changing community perceptions of HIV/AIDS is an important first step that leaders felt ill equipped to address. Future interventions must work with religious leaders to develop and implement Church-based interventions to reduce stigma.30,42 The most powerful methods for change are organic, community-based approaches, rather than externally-imposed strategies.29
Leaders in this study recognized their need for additional education and training to be able to offer appropriate HIV counselling, HIV specific ministries and support services, in addition to knowing how to help reduce stigma. They call for assistance in these efforts and saw the need for working together to share information and support one another in these endeavours, regardless of Church affiliation or beliefs.
Limitations
This study was subject to notable limitations. First, combining the various Christian-based denominations allowed for identifying common themes around sexuality and HIV stigma; however, it must be noted that there are myriad differences in the regulations, doctrines and practices of the multiple Churches within the Christian faith. Second, religious leaders’ willingness to participate in a study about religion and HIV/AIDS might also reflect their own desire to address the issue, leading to potential selection bias. Finally, it is important to re-iterate the inherent bias of the leaders interviewed who do not want to be seen as lacking compassion, an issue addressed by triangulating data both from interviews and a self-completed stigma scale. These limitations within the religious settings can potentially be built upon to recruit leaders for future interventions, as they indicate that1: there are Religious leaders willing to address HIV/AIDS despite existing stigma and doctrinal differences; and2 regardless of their personal and/or religious beliefs about HIV and PLWHA, there is a general desire and even a mandate to be compassionate and provide assistance to PLWHA.
CONCLUSIONS
With individuals living longer with HIV due to access to free treatment, there is an increased need for helping ensure their social, physical and emotional wellbeing. Low rates of disclosure and perceived stigma have been shown to lead to poor mental health, social isolation, poor adherence to treatment, greater risk for transmission of HIV, and higher rates of AIDS. The Church community can serve as the epicentre for improving the lives of persons infected with HIV. In this study, Christian religious leaders in Soweto view themselves as responsible for serving as mediators for PLWHA among their family and community, for educating their congregations about various HIV related issues, and for helping PLWHA restore their faith through repentance and forgiveness. HIV and religion continue to be tightly intertwined, indicating the necessity of involving the Christian religious leaders in efforts to improve the lives of individuals living with HIV/AIDS in Black communities. Considering the large Muslim religious community and the co-existence of traditional faiths and practices in Africa, future studies should seek to understand their similarities and differences with the Christian communities in order to broaden the reach of future interventions. The commonalities between Christian religious leaders in Black communities in sub-Saharan Africa and in the Americas facilitate the sharing of best practices and successful interventions for improving the wellbeing of PLWHA.
Acknowledgements
Our heartfelt thanks to the religious leaders in Soweto for sharing their thoughts with us and for their passion for serving their community.
Ethical considerations
%he University of the Witwatersrand, Johannesburg, South Africa, and the University of Rochester’s Research Subject Review Board, New York, approved study procedures.
Funding
This study was funded by a pilot grant from the University of Rochester Center for AIDS Research Grant P30 AI078498 (NIH/NIAID).
Competing interests
All authors have completed the Unified Competing Interest form at http://www.icmje.org/coi_disclosure.pdf (available on request from the corresponding author), and declare no conflict of interest.
Correspondence to:
Amina P. Alio, PhD
Associate Professor
Department of Public Health
University of Rochester Medical Center
265 Crittenden Blvd, CU 420644
Rochester, NY 14620
USA
[email protected]