According to the World Health Organization (WHO), the most common nutrient-related cause of anemia is inadequacy of dietary iron.1 In children, chronic iron deficiency anemia (IDA) can impair cognitive ability, growth, and development.2 During pregnancy, IDA increases risk of delivering babies preterm and subsequent low birth weights, reduces fetal iron stores, and infants born to women with IDA have greater potential to become anemic themselves.3 In developed countries, screening for IDA is routine, and for those with impaired iron status, a combination of dietary intervention and oral iron therapy is typically recommended. However, in regions of the world where populations are at greatest risk for IDA, barriers make IDA screening and subsequent treatment particularly challenging. For example, even though point-of-care, noninvasive field-tested devices are available to assess iron status, it can be difficult for healthcare workers to gain access to rural, secluded communities. It is likely, therefore, that the prevalence of IDA in these regions is higher than current estimates. Even when testing is possible, distribution of iron supplements provides only a short-term solution because those living in rural, impoverished regions lack the access and financial resources to purchase iron-rich foods or dietary supplements. Even governmental interventions such as iron fortification of indigenous staple foods such as maize and rice have proven difficult to implement because of economic constraints.4 For these reasons, IDA remains one of the most common, yet treatable, nutrition-related health problems in developing countries.
A new approach to IDA remediation, called Lucky Iron Fish®, overcomes many of these challenges. The Lucky Iron Fish (LIF) utilizes methodology similar to the time-tested intervention of using cast iron cookware to increase the overall iron content of food. When placed into a pot of boiling, acidified water for 10 minutes, this reusable, fish-shaped ingot releases iron into the cooking water. Subsequently, the food absorbs the iron from the iron-enriched water, increasing the overall iron content of the meal. It has been estimated that one meal prepared with a LIF can substantially contribute to overall daily iron requirements. Most importantly, LIF are reusable, and last for up to 5 years.5
The efficacy of the LIF has already been shown to improve iron status, at least short-term, among those consuming traditional Cambodian diets. In these randomized controlled trials, blood iron levels were higher among those preparing meals with a LIF compared to controls, although it is unclear if these improvements were sustainable over time.6,7 Clearly, studies of longer duration are needed to demonstrate the efficacy of LIF in reversing IDA, as well as assessing the use and success of LIF in other cultures that have dietary patterns that differ from those previously studied.
Therefore, the purpose of this study, conducted in rural, impoverished (7,750 by purchasing power parity; equivalent to 41% of the world’s average) regions of Guatemala, was to distribute LIF to those with impaired iron status to determine whether or not regular use of the LIF resulted in significant improvement in iron status (hemoglobin and hematocrit) after 12 months of use. This study was designed to address the following research questions:
-
Was there a significant improvement in iron status (hemoglobin and hematocrit) after 12 months of using the LIF on a regular basis?
-
What was the compliance rate for use of the LIF?
METHODS
This 52-week longitudinal study was implemented to assess changes in iron status (hemoglobin and hematocrit) after 1 year of using a LIF for meal preparation. Because of ethical considerations associated with withholding treatment and the potential to improve iron status, a control group for comparison purposes was not utilized. The study was conducted in collaboration with Hearts in Motion, a non-profit organization that provides free medical and dental care to people living in rural, underserved, and impoverished regions of Guatemala (all within a 300 km radius of Zacapa, Guatemala).
To provide contextual background, the majority of the population consisted of Spanish-speaking Latinos/Latinas, a mix of mestizo or Hispanicized peoples. However, some traces of indigenous cultures were present as evident by dress, linguistic traces, and customs. Guatemala has one of the highest inequality indexes; ranked 13th out of 111 countries evaluated by the United Nations Development Program.8 The birth, death, infant mortality, and fertility rates in this particular region of Guatemala are among the highest. Thousands of those living in poor, rural communities migrate seasonally to harvest crops or to seek employment in urban regions.9 The town of Zacapa, the main center of operations for the Hearts in Motion organization, is mainly rural and is located in the eastern part of the country.
During this 7-day medical mission, a total of 302 people living in 3 different villages were screened for iron deficiency anemia. Village 1 is a mainly rural settlement, and the surrounding areas are extremely poor, with scant resources in terms of access to clean water or electricity. The vast majority of those living in Village 2 were able to read and write, although most lived in the rural portion of this municipality; approximately 124 square km. Village 3 was also located in a rural setting, but had a 3-room house that served as a small health and social center. It was noted that many participants share the same last names, suggesting that families tend to remain on site, and are secluded from other communities. Of the 302 people screened for IDA, 46.7% (n=149) had impaired iron status (based on hemoglobin, hematocrit, or both) as determined by World Health Organization (WHO) standards (Table 1).
To assess iron status, a small amount of blood (10–20 microliter) was obtained using Accu-Chek Safe-T-Pro disposable lancets (Roche Diagnostics, Indianapolis, Indiana, IN, USA). A capillary tube and a cuvette were filled with blood, obtained by gently massaging the finger. The HemoCue® Hb 201 System (HemoCue America, Brea, California, CA, USA) was used to measure hemoglobin (g/dL), and a battery-operated micro-centrifuge (HemataStat II) (EKF Diagnostics for Life, Boerne, Texas, TX, USA] was used to measure hematocrit values (%). Quality control measures using known standards were used to ensure instrumentation consistency prior to screening. Information regarding age, sex, women’s reproductive status, number of children living in a household, meat (beef, poultry, and/or fish) consumption, weight, and height was also collected. The use of tobacco products and alcohol consumption was infrequent in this population, which was likely due to cultural factors, a lack of accessibility and limited financial means. Subjects were living at sea level thus adjustment of data on blood hemoglobin concentrations was not necessary.
There were no eligibility requirements to participate in this study, other than being 5 years of age or older and meeting the WHO criteria for IDA (hemoglobin, hematocrit, or both). Subjects with IDA at baseline (week 0) were asked to participate in the study. Subjects were told that if they consumed daily meals prepared with a LIF and then returned 1 year later to have their iron status retested, they would receive 38 Guatemalan Quetzals, equivalent to US$5 dollars. Subjects were required to bring their LIF when returning to be retested for the purpose of identity verification. All (100%) of the people that were screened and met the criteria for IDA agreed to participate in the study. Parental/guardian consent was obtained to enroll children in the study.
Adult subjects indicated informed consent by signing the study consent form. If subjects were unable to read, the consent form was read out loud, and for those unable to write, signing the letter “X” indicated permission. Parental/guardian consent was obtained to enroll children (≥5 years) in the study. Once study consent was obtained, subjects completed a short questionnaire (biographical information), and then anthropometric measures (weight and height) were taken. All procedures were reviewed and approved by the Washington State University Institutional Review Board.
For the purpose of this research, it was important to identify the person responsible for preparing family meals, designated as “head of household.” This was necessary for two reasons: 1) it is erroneous to assume that the person preparing household, daily meals was the parent because it is typical in rural, impoverished regions of Guatemala for multi-generational families to live and share daily meals together; and 2) the average age to marry and have children is 15 years. Thus, it is possible that the designated head of household may be someone much younger than would be expected in the US and someone other than the parent. Although the head of household may or may not have impaired iron status, this step was necessary because the head of household was the person responsible for using the LIF in meal preparation. Therefore, the person identified as head of household received training on preparing meals using the LIF, and may or may not have been enrolled in the study.
Heads of households were instructed (in Spanish) how to prepare meals using a LIF. Meals were to be prepared by placing the LIF and one vitamin C tablet (250 mg for the purpose of water acidification) into a pot of boiling water for 10 minutes. Subjects were told that the “tablet” was necessary to “feed” the fish. After removing the LIF from the boiling water, subjects were told to add other meal components, mostly beans and rice, to the iron-enriched water. Heads of households were asked to prepare at least one daily meal using the LIF. Once the 15-minute educational session was complete, each participant was given laminated illustrative instructions on the use of the LIF to take home, one LIF identified by subject number, and 365 vitamin C tablets (250 mg) for the purpose of water acidification. Subjects were told that study personnel would return to retest their iron status (post-intervention; week 52).
Approximately 1 year later, study personnel returned to each village to assess iron status. Blood collection measures were repeated using the same instrumentation as used during the baseline measurements. A paired t test was used to determine if there was a significant difference (P≤0.05) between measures of iron status (hemoglobin and hematocrit) at baseline (week 0) and post-intervention (week 52).
RESULTS
Screening and baseline
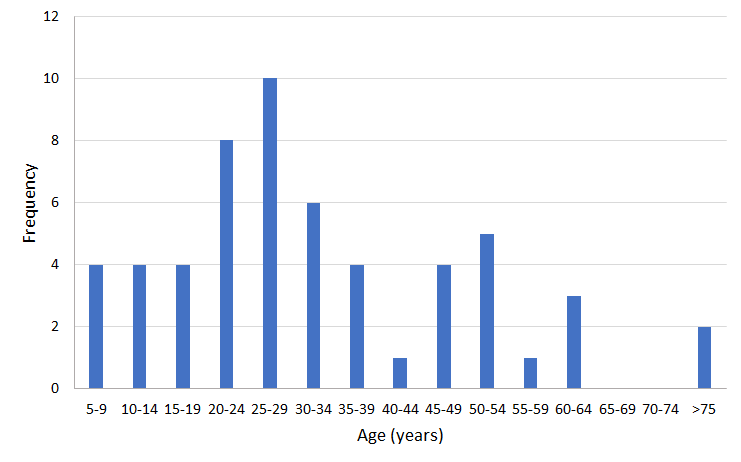
A total of 302 people (257 females; 85% and 45 males; 15%) were screened for IDA (Table 2). Of these, 145 (48.0%) met the WHO standards (based on levels of hemoglobin, hematocrit, or both) for IDA. Of the 257 females that were screened for IDA, 46.3% (n=119) were determined to have IDA, compared to 27 (60.0%) of males. A total of 24 (42.9%) subjects were below WHO criteria for IDA based on hematocrit only, 9 (16%) of subjects were considered to have IDA based on hemoglobin (g/dL) values only, and 23 (41%) subjects were below WHO criteria for IDA based on both hemoglobin (g/dL) and hematocrit (%) values. The average age of those screened for IDA ranged from 5 to 81 years, with a mean age 32.38 ±17.7 years for those with IDA, compared to 25±17.7 years for those without. Probability analysis determined that the age distribution (Figure 1) fit a normal curve, both with and without outliers older than 60 and younger than 10 years. A contingency table comparing the prevalence IDA by village (Pearson χ2=0.140, DF=2, P=0.932) indicated no differences. Self-report estimates of meat consumption indicate that beef, poultry, and/or fish are consumed infrequently, and that the majority of subjects (n=40; 71.4%) lived in households that had an average of 3.75 children still living at home.

Post-intervention
A total of 49 (41.1%) of females and 7 (25.9%) of males with IDA at baseline returned to have their iron status retested. Logistic regression was used to determine if the two periods were significant in predicting the presence or absence of IDA, using individual as a random effect in the model. It was found that there was little variation caused by individual and that the odds of not having anemia were significantly higher at week 52 compared to week 0 (P<0.001). For subjects that were measured at baseline, 45 (80.3%) were no longer anemic at week 52, with a mean difference (week 52 being higher than baseline) in hemoglobin of 1.28 (19.6% improvement) and a mean difference in hematocrit of 3.8 (28.5% improvement). A total of 11 subjects (19.65%) remained anemic at 52 weeks. A paired t test using all data points showed that mean differences in both hematocrit (g/dL) and hemoglobin (%) values were significantly higher post-intervention (P<0.001 for both) (Table 3). Further analysis (n=46), excluding pregnant women, individuals ≥60 (y), and children ≤10 years of age as potential outliers, showed similar results (Table 4).
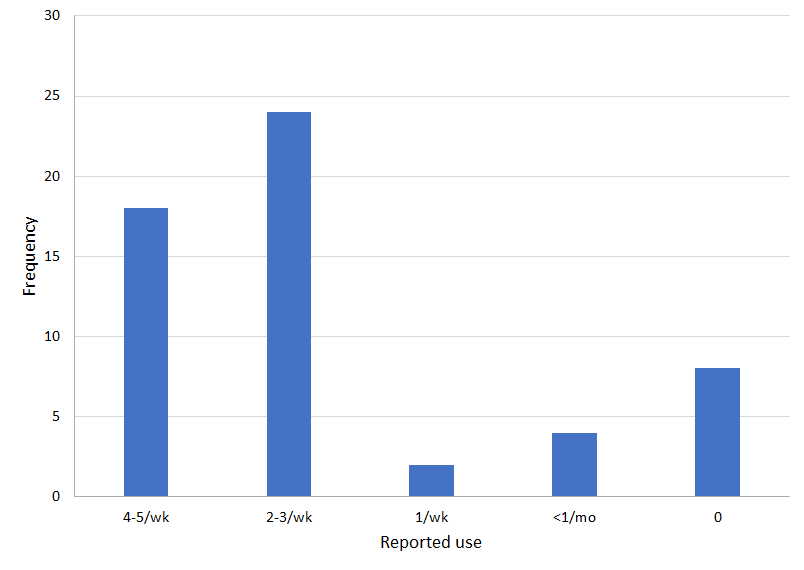
The majority of subjects (75%) reported using the LIF at least twice a week, and only 3% reported using it once a month. Of the subjects that remained anemic (n=11), 2 reported using the LIF infrequently (<1/month), whereas 89% of those reporting frequent use (≥2/week) of the LIF were no longer anemic. In general, as people used the LIF more frequently, the less likely they were to remain anemic. However, when categorized by reported frequency of LIF use, sample size was insufficient for statistical comparison (Figure 2).

DISCUSSION
The primary objective of this study was to demonstrate improvements in iron status (change in hematocrit (g/dL) and hemoglobin (%) values) after 12 months of consuming meals prepared with a LIF. Among those that reported frequent (≥2/week) LIF use, there was a demonstrated statistically significant increase in both hematocrit (g/dL) and hemoglobin (%) values. Although this study did not utilize an experimental design (eg, a control group and randomization), the results strongly suggest that the LIF is efficacious in improving iron status in regions where IDA prevalence is high.
An additional study objective was to determine the compatibility of using a LIF in a population with dietary patterns and cultural food practices different from those previously studied.6 It appears that preparing foods such as black beans and rice, which are the primary food staples in Guatemala, is compatible with meal preparation using the LIF. The majority of subjects (nearly 89%) reported using the LIF at least 2/week to prepare meals over the 52-week period. Although occasional use of a LIF alone is not enough to entirely satisfy daily iron requirements, overtime it appears to provide enough additional iron to diets that are otherwise severely lacking this important nutrient.
Also important to note is that this study was able to reach a population that is difficult to access; that is adults and children living in rural regions of Guatemala. As such, estimates of iron deficiency anemia were higher than those reported by other studies and agencies. Although this study did not include children under 5 years of age, studies that included younger children (< 3 years of age) have also reported a high occurrence of IDA, with 38% having hemoglobin values below 11 g/dL.8 Thus, the high prevalence of IDA observed in this study suggests that IDA is a health problem of greater magnitude than previously reported. Currently, IDA is considered a moderate public health problem in Guatemala, with reported prevalence rates ranging from 21.4% to 38.3%.10 By comparison, of the 302 people tested in this study, the occurrence of IDA among adults and children (≥5 years of age) was nearly 50%, and according to WHO thresholds is considered severe.11 As IDA may vary regionally, studies to compare IDA rates in other locales would be of great importance.
It is duly noted that study results are based on a relatively small sample size (n=302) and reflective of a specific region of Guatemala. However, these villages are not highly populated areas, but rather rural and secluded, far away from urban centers. It is therefore likely that those that volunteered to have their blood tested for IDA provided a fairly representative sample, with the exception of adult males. Adult males are less likely to attend medical clinics because they typically are working during the day, whereas women and children are likely to be more available. It is also unlikely that subjects self-selected to attend medical clinic for the sole purpose of having their iron status tested (self-selection bias). Rather, access to any medical and dental care is so infrequent that villagers attend clinics for nonspecific reasons. In fact, the concept of IDA was not familiar to subjects, and therefore had to be explained in very general terms.
Of those enrolled in the study (n=145), less than one-half (38%) returned at week 52 to be retested. It is difficult to ascertain the exact reasons for the low number of subjects in the follow-up sample. It is certainly possible that those given a LIF to prepare meals (week 0) simply did not comply with study protocol, which could be viewed as a potential source of compliance bias. For this reason, it is important to determine whether the LIF proved difficult to use and/or was viewed as culturally inappropriate. Superstitious beliefs are a part of Guatemalan culture, and unfamiliar objects could be perceived as having bad spirits. In Cambodia, where the idea of the Lucky Iron Fish first originated, fish are symbolic of good luck and associated with health and happiness. In Guatemala, fish may represent something different, and therefore the acceptability of a fish-shaped ingot may warrant further investigation.
Also in regards to the low return rate, it is important to consider that typical means of communication used to remind subjects for study follow-ups were not available (eg, telephone, mail, and internet), thus we relied solely on word-of-mouth. Furthermore, subjects had to walk to a central location, sometimes miles away, which also demonstrates commitment (or lack thereof) to the study. It is also possible that children enrolled in the study were in school or working the day study personnel returned for retesting. Furthermore, study participants could have fallen ill or perhaps had died. Although speculative, these are all reasonable explanations for noncompliance. Therefore, it is difficult to ascertain why 62% of those enrolled in the study did not return to be retested. However, after considering all the various reasons why people may not have returned (noncompliance), a nearly 38% return rate was considered adequate to test the efficacy of the LIF in remediation of IDA.
It has been estimated that only a small percent (2%) of school-age children in Guatemala consume diets that provide adequate amounts of iron.8 The results of this and other studies12 suggest regular use of a LIF for meal preparation offers a safe and effective means to reverse IDA, provides an additional source of dietary iron that otherwise might be lacking, and can replenish the body’s iron reserves. Since iron deficiency anemia tends to run in families, all family members are likely to benefit from this intervention. Unlike developed countries where iron-rich food sources are abundant, government food fortification interventions exist, and oral iron supplementation options are readily available and affordable, alternatives such as these are not feasible in countries such as Guatemala. Although subjects were not asked about dietary practices at follow-up, it is unlikely that subjects’ diets changed over the course of 52 weeks due to limited food accessibility and financial means. Black beans, white rice, corn tortillas, and coffee remain the primary food staples in Guatemala, none of which provide significant amounts of iron. Therefore, we attribute the improvements in iron status to the use of the LIF, and not to changes in dietary practices.
Further investigation is warranted before a widespread, sustainable LIF program can be implemented in Guatemala. For example, the release of iron from a LIF is highly dependent on proper water acidification, which could be problematic. There is a need to research available food sources in rural, impoverished regions of Guatemala that could serve as acidifying agents. In the eastern region of Guatemala, very few foods are acidic enough to obtain a critical pH of 4.5; the minimum value needed for iron release from the LIF. Once these resources are in place, efforts should be made to implement far-reaching studies to further test the efficacy of the LIF in other regions of Guatemala.
CONCLUSION
In conclusion, regular use of the LIF in food preparation may substantially and safely contribute to overall daily iron intake in rural, impoverished regions of Guatemala where adequate dietary intake of iron may be problematic. Promoting dietary change in remote populations is not feasible due to a lack of affordable, accessible iron-rich foods. As such, the LIF offers an easy way to improve the nutritional value of daily meals. Furthermore, using the LIF empowers those without the financial means to take steps to improve their own health. However, for widespread implementation to be successful, there is a need for health officials to provide educational support and to incentivize the population.
An inability to follow-up with subjects after the initial enrollment in the study likely contributed to the low response for retesting. Nonetheless, this study offered important insights regarding a novel approach to treat IDA. Short-term fixes such as iron supplements do not encourage people to be active partners in self-care, and are not long-term solutions to a chronic health problem. By encouraging people to invest in the solution (using their Lucky Iron Fish on a regular basis), outcomes (improved iron status) are likely to be more successful.
Acknowledgements
The authors greatly appreciate those that assisted with this study. First and foremost, the authors express their gratitude to Lucky Iron Fish® (Dr. Alastair Summerlee and Lydia Summerlee) for their guidance and support throughout this project. Secondly, we acknowledge Hearts In Motion (Karen Scheeringa Parra, Julie Gilliam and Bert Echeverria) for making this project possible. Hearts In Motion provides medical and dental care to underserved communities in Guatemala. We are also greatly indebted to those that assisted with data collection during the medical mission. In particular, we want to thank the Washington State University students (Nelly Avila, Philip Behrend, Courtney Cahill, Mike Cahill, Hailey Cates, Vikram Chandra, Michael Cofano, Anthony Deleon, Blake Ellingsen Taylor Ellingsen, Mazmin Escalera-Mendea, Ryan Feser, Noah Hunthausen, Denali Kagel, Joanne Kunze, Kaelin Moya, Mariela Olivares-Gutierrez, Adilene Palencia, Stephanie Riley, Mia Ryckman, Natasha Saric, Kiya Savochka, Molly Shipman, Miguel Sotelo, Ryan Voelker, Girard Watson, McKenzie Webb, Danielle White, and Joshua Wilkes). In addition, we recognize Chris Cotton, Dianalyn Ouellette, Evan Klein, Alivia Stoddard, Aanya Lall, and Neha Lall for their assistance with data collection and other related contributions.
Disclaimer
Although Lucky Iron Fish® donated the Lucky Iron Fish for the purpose of this study, the findings and conclusions are those of the authors.
Funding
There was no monetary funding source, although Lucky Iron Fish donated 200 Lucky Iron Fish for the purpose of this study.
Conflict of interest
The authors have completed the Unified Competing Interest form at http://www.icmje.org/coi_disclosure.pdf (available on request from the corresponding author) and declare no conflict of interest.
Correspondence to:
Kathy Beerman
School of Biological Sciences
Washington State University
Pullman, Washington 99164
United States of America
[email protected]