
Access to freshwater is indispensable for drinking, hygiene, and other essential livelihood activities. However, across the world’s major river deltas, such as the densely populated Ganges, Nile, and Mekong deltas, freshwater sources are threatened by global environmental change and non-climatic factors. In these areas, patterns of land use, changes in water management in upstream watersheds, and sea level rise have contributed to increasing salinity and saltwater intrusion, a process by which seawater intrudes inland into freshwater sources.1–6 Successful adaptation to the impacts of salinity in surface and groundwater has therefore become a matter of survival. This situation motivates the current study, which hones in on Bangladesh’s southwest coastal region to derive insights for adapting to salinity-induced freshwater scarcity. Although the term, ‘adaptation,’ has a specific connotation in the context of climate change,7 it is used here to refer to actions to moderate or avoid harm associated with the effects of salinity as an environmental phenomenon, notwithstanding its non-climatic drivers.
Situated in the Ganges-Brahmaputra-Meghna delta, the southwest coastal region of Bangladesh is a prime example of a region vulnerable to increasing salinity. Investigations have reported surface and groundwater sources as significantly more saline than levels acceptable for consumption.8–13 While salinity varies greatly by season, year, and location, there is an overall upward trend. Studies note increases in average yearly salinity14 and highest recorded salinity levels9,15 of specific water sources. The saline water front is projected to move further inland, and salinity is expected to intensify.9,16–18 Various environmental and manmade factors play a role in driving salinity, and the relative importance of a given factor is a contentious matter addressed elsewhere.19 Drivers cited in the literature include saltwater shrimp farming,20–25 diversion of the Ganges river upstream by India’s Farakka dam,15,26,27 and sea level rise among other climate impacts.2,28,29 At the same time, heavy metal contamination of groundwater, especially by arsenic, persists as a serious concern, further exacerbating freshwater insecurity.30
In this context, the rural southwest coast faces the challenge of adapting to freshwater scarcity. Non-governmental organizations (NGOs) and other development actors have intervened to facilitate responses. Various adaptation technologies at the household and community levels exist, but their success and advantages/disadvantages are not well documented.
This study thus combines qualitative research and environmental testing to obtain an in-depth view of salinity-induced freshwater scarcity. It aims to document the impacts of salinity on various domestic water uses, including drinking, cooking, and hygiene. It studies how inhabitants are responding to these impacts and how development actors are assisting with adaptation. It analyzes the specific challenges associated with household- and community-level adaptation strategies. Our findings lay the groundwork for future quantitative studies and adaptation interventions that can be more attentive to the needs of low-resource deltaic settings in Bangladesh and beyond, which are grappling with salinity intrusion.
METHODS
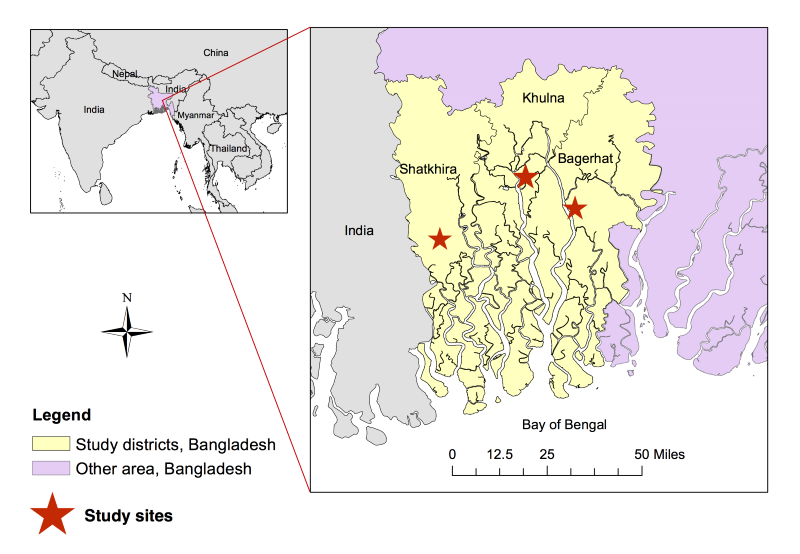
The study sites were three villages, purposively selected to represent the three southwest coastal districts of Bangladesh and to have moderate or high salinity, as measured during site selection in February 2015. The sites were located in the Dacope sub-district of Khulna District, the Mongla sub-district of Bagerhat District, and the Shyamnagar sub-district of Satkhira District (Figure 1).

Data collection
We conducted village-level data collection at the three sites and NGO-level data collection in the southwest coastal region and Dhaka city. Written consent was obtained from all participants. The study was approved by the Institutional Review Board of Johns Hopkins Bloomberg School of Public Health, and the Research Review Committee and the Ethics Review Committee of the International Centre for Diarrhoeal Disease Research, Bangladesh.
Phase 1 – Village-level data collection
There were two rounds of village-level data collection. The first round in May/June 2015 coincided with hot season and the beginning of rainy season. Across the three sites, researchers recruited 25 households with whom they conducted a structured half-day visit. The visit consisted of: two in-depth interviews with a male and female household member, a questionnaire, and salinity testing of the household’s sources of water (eg, household ponds, tubewells, piped water source). The research team measured electroconductivity (EC) as an indicator of salinity (see Appendix S1 in Online Supplementary Document(Online Supplementary Document) for the salinity testing protocol). The team also conducted six gender-specific focus groups, interviewed ten community key informants (eg, village leaders, NGO fieldworkers), and tested the salinity of community-level sources of water (eg, community tubewells and ponds, canals). In total, qualitative data were obtained from 116 community members (63 females, 53 males).
The second round of village-level data collection took place in October 2015, in mid-to-late rainy season. The team revisited recruited households, administered a follow-up questionnaire, and conducted a follow-up interview with one household member. It also measured the salinity of water sources previously tested.
Phase 2 – Stakeholder-level data collection
The second phase, conducted in January/February 2016, involved in-depth interviews with 24 informants across 16 different NGOs. The NGOs consisted of four local organizations, four national organizations, and eight international organizations.
Data analysis
Salinity testing results were graphed and mapped. Household questionnaires were tabulated. Interviews and focus groups, which averaged two hours and three hours, respectively, were audio recorded and transcribed. Transcripts in Bangla were translated into English. Transcript-by-transcript analysis entailed: (a) coding notable quotes with MaxQDA v11 (VERBI GmbH, Berlin, Germany), based on codebooks following the major topics of each activity; (b) extracting information into a summary document based on a template; and (c) updating a memo of cross-cutting observations. Findings were synthesized using these three components.
RESULTS
Salinity testing
Salinity testing of 37 surface water sources (ponds, streams, canals) and 8 groundwater sources (tubewells reported as 200 feet deep or less) revealed high salinity and wide spatial and seasonal variation. As points of comparison, Bangladesh’s Water Resources Planning Organization establishes a target threshold salinity of 2000 μS/cm for groundwater in the region,31 while the US Environmental Protection Agency sets a drinking water guideline of 500 mg/L for total dissolved solids (roughly 1000 μS/cm, if all TDS were sodium chloride).32
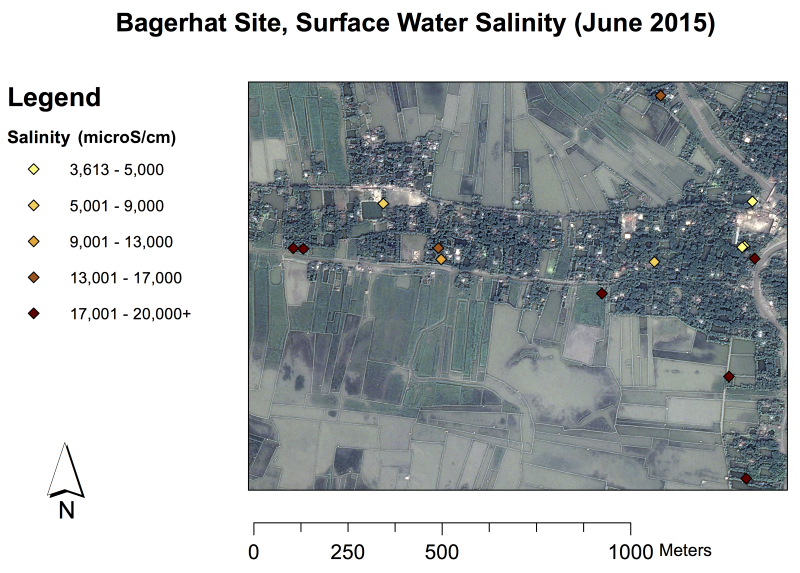
Surface water measurements in June, corresponding to hot season and the beginning of rainy season, ranged from 3613 to over 19999 μS/cm in Bagerhat, 1347 to over 19 999 μS/cm in Satkhira, and 1049 to over 19 999 μS/cm in Khulna (the upper limit of the meter used was 19999 μS/cm). Salinity values measured in October 2015 were much lower: 825 to 3998 μS/cm in Bagerhat, 715 to 7595 μS/cm in Satkhira, and 650 to 4890 μS/cm in Khulna. Figure 2 graphs the salinity of surface water sources sampled by season and study site. Each bar of a particular shading and position represents a unique source sampled within a given study site at two separate times; i.e., the first bar in Bagerhat shows a source that measured 18 500 μS/cm in June, which decreased to about 1000 μS/cm in October. Moreover, it appeared that salinity could be quite localized, i.e., with disparate values for relatively proximate locations (Figure 3). Additional maps are provided in Appendix S2 of Online Supplementary Document(Online Supplementary Document).


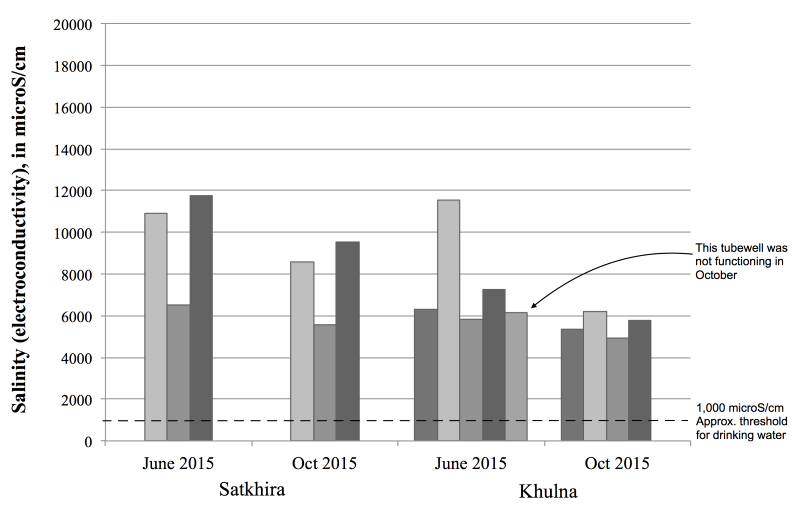
For groundwater, salinity in June ranged from 6520 to 11 747 μS/cm in Satkhira, and 5822 to 11 527 μS/cm in Khulna. Values were slightly lower in October. Figure 4 graphs the salinity of groundwater sources by season and site; again, each bar of a particular shading represents a unique source sampled within a given site.

Local perspectives on the impacts of salinity on access to water
Salinity in groundwater and surface water contributed to water scarcity across the three sites. Participants maintained that relatively few tubewells were built in their communities because of groundwater salinity. In fact, the research team found no functional tubewells at the Bagerhat site. For those tubewells that had been constructed, participants frequently reported that the water was too salty to consume, and could only be used for hygiene, routine housework, and occasionally livestock and irrigation. Surface water sources were unable to alleviate freshwater scarcity. Participants reported that several decades earlier, ponds contained freshwater, but grew saline due to saltwater infiltration from neighboring shrimp ponds.
There was, however, notable seasonal variation. According to study participants, hot season, roughly March to June, was the most saline season and corresponded to the most severe impacts. Salinity was perceived to decrease starting with rainy season in June, hitting a low at the end of rainy season in October. It then rose with the coming of winter, through winter (roughly October/November to February) and into hot season.
Household questionnaires, which assessed the sources of water used throughout the year, confirmed the seasonal nature of salinity’s impacts (Table 1). (Note that many households reported using more than one source of water for a given purpose, thus percentages may add up to more than 100%). Drier seasons – winter and hot season – obligated households to resort to more distant sources of water for all purposes, but especially drinking. For example, in rainy season, nearly all households collected rainwater in earthen pots and plastic containers to consume. Only 4 out of 25 households reported having to travel outside the village to retrieve drinking water to supplement the rainwater collected at home. In contrast, in winter and hot season, 15 of 25 households had to access drinking water from a source outside the village, with 9 of these households reporting that this was their only source of drinking water.
For hygiene, the large majority of households used ponds within their homestead for bathing during rainy season. In winter and hot season, several of these households used ponds elsewhere or tubewell water for bathing, however most households continued to bathe in their own ponds.
The questionnaire data on the usage of tubewells and rainwater-harvesting (RWH) tanks also confirmed the narrative accounts given by study participants – that such infrastructure was less available and hence less often used throughout the year.
Information from the questionnaires and salinity testing was triangulated to document salinity of some of the water sources used in the study area, which were sampled by the research team. During hot season, multiple sources of water were being used for drinking ranging 3000 to 7000 μS/cm, and for cooking ranging 4000 to 11 000 μS/cm. Many sources used for bathing in hot season measured over 10 000 μS/cm, with a few exceeding 19 999 μS/cm (the instrument’s limit).
Consumption of saline water was frequently linked to gastrointestinal symptoms, including diarrhea, vomiting, upset stomach, loss of appetite, and irritation/bleeding in the throat. Some participants also mentioned thirst. Several reported that cooking with saline water rendered food inedible.
Use of saltwater for bathing and other personal hygiene was frequently associated with itchy, irritated skin and eyes, and darkening complexion. Various participants noted that it was not possible to lather soap with saltwater. Several linked poor hygiene to skin rashes and scabies. There were also reports of refraining from using the latrine due to lack of freshwater for cleaning afterwards.
Options and challenges in adapting to salinity’s impact on water
Inhabitants and NGO representatives discussed several strategies for acquiring and/or storing freshwater in the context of salinity: RWH, ponds, paying for water delivery, tubewells, managed aquifer recharge (MAR) systems, and desalination.
Rainwater-harvesting
Inhabitants generally viewed rainwater as the best option for drinking water, in terms of purity and aesthetics. All households collected rainwater using small, plastic containers and earthen jugs, known as maith. However, maith only supplied a family with a couple days’ worth of drinking water. Villagers universally expressed a preference for large (1000+ L) RWH tanks, suitable for storing water collected off of tin-roofed dwellings.
In the study area, both plastic and concrete RWH tanks were found. Concrete RWH tanks tended to be larger, supplying clusters of households. Beyond technical flaws (like poor durability of concrete and overheating of plastic tanks), the most frequently cited barrier with respect to RWH tanks was their cost. Plastic tanks, for example, cost US$100 to US$200. Few middle-class and poor households had access to them. As a woman from Bagerhat remarked, “We work as daily laborers… Are people like us capable of buying a 2000-litre water tank? No, we don’t have that capacity. We are barely eating three times a day.”
Across the sites, various NGOs provided assistance in procuring RWH tanks. However, help was described as vastly insufficient. When NGO assistance took the form of a loan, it was usually only offered to members of the NGO’s samity (a cooperative group where members made regular savings deposits and applied for loans). Moreover, not all samity members could afford a loan. When NGOs provided RWH tanks on a cost-sharing basis (which was still inaccessible to the very poor) or completely free (which was rare, because NGOs predominantly thought ‘handouts’ would be undervalued), the widespread community perception was that tanks were not distributed according to need. Numerous villagers pointed to nepotism by local politicians, who helped name tank recipients. They echoed the sentiment, as expressed by one inhabitant:
“Aid is provided to their [local politicians’] relatives mostly… [I]f the tanks are given through the [union] chairman and [ward] member…the house that already has one will get three, and the house without any will not get a single one.”
Joint ownership was a contentious issue related to RWH tanks. NGO representatives generally thought it unfeasible to provide a RWH tank to each household. In some cases, NGOs constructed a larger concrete tank at the site of one household, to be shared among that household and its neighbors. However, many villagers expressed concern that others would take a disproportionate amount of water and/or misuse water for purposes besides drinking. Moreover, they pointed to cases where a household, which had agreed to share an NGO-provided tank with its neighbors, ceased to share after the NGO stopped monitoring. Community key informants who had worked on NGO tank programs confirmed this problem, with one rationalizing the beneficiary’s position as follows: “The scarcity of water in this area is severe…If I have plenty, I will not hesitate to give you some. But when I am in need, I will not want to give you any.” One villager suggested that a guardian could be appointed to each multi-household tank, but most respondents insisted on individual household ownership.
Ponds
In the absence of fresh groundwater and enough stored rainwater to last the year many inhabitants resorted to pondwater for drinking, cooking, and other purposes. All ponds encountered in the study area were affected by salinity to some extent, in varying degrees (see Figure 1). Aside from salinity, participants noted several major problems with ponds: travel time, bad odors, dirtiness (from algae, animal waste, dead vegetation, and other contaminants), and low water levels in hot season.
In order to access a pond that was less saline, had a filter installed, or was deep enough to still have water through hot season, many inhabitants traveled outside their household (or village) or paid someone to deliver that pondwater. Fetching water caused muscle and joint pain, increased risk, and detracted from income-generating activities. For example, one woman from Satkhira described her trips to a pond in a neighboring village. It took half an hour to bring one large urn of water, and her family required four or five daily. Several women reported that fetching water was so burdensome that they would make the water last longer by mixing it with saline water found nearby.
Pondwater quality was another problem. Some villagers filtered pondwater using a strainer or alum (potassium aluminum sulfate, known locally as fitkari), mostly to filter out dirt. Using chlorine and boiling water did not appear common. Some inhabitants reported that pondwater was especially contaminated in the hot season, and perceived greater incidence of diarrhea, dysentery, and other waterborne diseases then. Given salinity and contamination, pondwater was often used only for washing and cleaning.
The research team observed one intervention – a pond sand filter (PSF) system – intended to improve pond infrastructure at the community level. The typical intervention consisted of an NGO (or sometimes the government) finding or excavating a large pond that was relatively less saline, reinforcing an earthen embankment around it, and installing a system to pump pondwater through a sand filter and into a storage tank with faucets. Among NGOs, communal PSFs were popular given that they could, in theory, service an entire community cost-effectively. There were several challenges associated with community PSF systems, however, rendering it the least desirable adaptation strategy to residents across the study sites.
Firstly, finding an appropriate location was difficult. The area had to be insulated from saltwater, at present and long-term. Publicly owned land was not always available, and private landholdings were often fragmented. If situated on private property, the landowner had to agree to communal use of his land.
Moreover, PSF systems drew users from surrounding villages, leading to crowds and lines for a free faucet. As one woman stated: “People come from everywhere…. Dusk may come, so to save time and be able to come home quickly, I’ll take water directly from the pond.”
One of the most significant challenges, noted by villagers and NGO workers who had implemented PSFs, was keeping the system operational. In addition to normal wear and tear, storms, flooding, and other natural hazards could also damage PSFs. Participants reported that frequently, nobody took responsibility for cleaning and repairing the filter. Even NGOs that had installed many of these systems doubted their long-term functionality. As one representative remarked, "If there are ten PSFs developed by the government and ten developed by NGOs, nine of those government ones are not working, and probably five of the NGO ones are working".
The maintenance issue appeared related to collective action and responsibility, rather than money. Some NGOs reported that they had left the community with tools for maintenance and repair, but the tasks went uncompleted. One NGO representative recounted, and others echoed, attempts to engage communities:
"It’s not expensive to clean the filter media…. But in our culture, who will do it is the big challenge. NGOs like us, we have been trying for a number of years to make communities understand…. [T]he communities’ mindset is like this: someone came and built this here, so it’s their responsibility for cleaning it."
While NGO representatives readily spoke of obligations that fell to villagers, they rarely addressed the accountability of state actors unless specifically asked. The potential for coordinating with local government was viewed with skepticism, given the centralization of power in Bangladesh and perceived unwillingness of local government to assume new responsibilities. One informant with three decades of experience with a national NGO elaborated that political officials at the union level “avoided responsibility by pointing to a shortage of manpower.” These officials did not take charge of infrastructure maintenance, neither for PSFs constructed by NGOs, nor for other infrastructure built by specialized government agencies, such as the Department of Public Health Engineering (DPHE).
Paying for water delivery
Paying for water delivery was another option used to obtain drinking and cooking water. The informal method consisted of paying a person with a bicycle-drawn cart to retrieve water from a source, typically a PSF system, superior to closer options. An alternative method, which some participants had observed in neighboring villages, consisted of piped water delivered to households or a distribution point in the village from an outside source. In some cases, water would be supplied only at certain times.
Most villagers who referenced a piped water system portrayed it positively, though awareness of the benefits and drawbacks of such a system appeared limited because they did not have first-hand experience using one. On the other hand, several NGO informants provided examples of families in other villages who refused to pay even a nominal fee for piped water. The families reportedly did not understand the advantages of an improved water source or felt water should be provided free.
Tubewells
The tubewells we observed were hand-pumped and shallow, with depths of 200 feet or less, and generally yielded water too saline for consumption. Salinity testing revealed that decreases in groundwater salinity between hot and rainy seasons were relatively minor (compare Figure 1 and Figure 3). The main advantage was that tubewell water was perceived as unlimited, and by the end of hot season other sources of water were depleted.
A few households reported walking to retrieve water from more distant, less saline tubewells. These were typically privately owned, but owners allowed others access and in some cases collected a small fee for maintenance. The tubewells were reported to attract so many people that there would almost always be a wait. However, tubewell owners were more willing to share because the water was perceived as unlimited.
Nevertheless, most participants across the sites doubted that constructing more tubewells would alleviate freshwater scarcity. They recounted that households, NGOs, and government actors had attempted to install tubewells in the past, but largely failed to find freshwater. Villagers suggested that were it possible to locate a freshwater aquifer, a deep tubewell would be the ideal adaptation – superior even to large RWH tanks because of its “unlimited” nature. (Arsenic in groundwater appeared to be a less salient concern in the study sites; however it was a significant concern at one of the candidate sites visited but not selected, where shallow tubewells yielded relatively fresh water).
Managed aquifer recharge (MAR) and desalination technologies
According to several NGO representatives, two other community-level options drawing on more advanced technology had potential to alleviate freshwater scarcity in salinity-affected areas. The first, known as a managed aquifer recharge (MAR) system, consisted of collecting rainwater during rainy season and using it to artificially recharge a shallow aquifer. The water, stored underground, would create a freshwater buffer from the aquifer’s typically brackish groundwater. The freshwater could then be extracted during other times of the year. During the study period, local universities and others were piloting MAR systems in the region. However, several NGO informants, including two who worked on the pilots, noted maintenance challenges similar to the difficulties in upkeep of PSFs. As upkeep of MAR systems was even more sophisticated than PSFs, this was a particular concern.
Reverse osmosis technology, a form of desalination, was also mentioned by a few organizations, but was perceived as impractical for widespread implementation in Bangladesh. The technology consisted of treating and pressurizing saltwater, then passing it through a water-permeable membrane to separate out the salts. However, according to several NGO representatives, the need for a large, stable energy supply was an obstacle.
DISCUSSION
This study sheds light on the significant extent of water insecurity resulting from salinity – a crisis obscured by survey data touting nearly universal access to ‘improved sources of drinking water’ across rural and urban Bangladesh.33 As Pal et al. warned in their evaluation of water management policies in Bangladesh, water and sanitation access statistics carry the “risk of giving a false sense of security, thereby diverting the attention of authorities from the pressing need” to prioritize water provision.34 Examining the impact of salinity on rural household water in Bagerhat, Satkhira, and Khulna, the combination of participant accounts with environmental and questionnaire data reveals high vulnerability, not only in terms of consuming saline water (which has been studied to some extent in the public health literature),10,11 but also with respect to bathing with water so saline it exceeded what could be measured. Even inhabitants who manage to procure relatively fresh drinking water appear vulnerable to the impacts of using saline water for hygiene. These include severe skin and eye irritation, poor personal hygiene, and refraining from relieving oneself.
This research complements prior studies and helps to contextualize their findings. For example, Benneyworth and colleagues surveyed 200 households in Khulna, and observed that an overwhelming majority of respondents did not perceive their water as having a bad or salty taste.8 However, their respondents did associate pondwater with poor water quality and salinity, and these findings now suggest that those characteristics would affect their hygiene outcomes. Moreover, while 81% of the respondents in their study manifested that a water collection trip took under twenty minutes, the researchers noted that the indicator did not consider seasonality or number of trips per day. The present study suggests that there is a much greater burden during the hot season and at least four or five trips are typically needed daily to supply a four-member household.
Recently, Rahman et al. examined drinking water scarcity among 200 households across Satkhira and documented diarrhea as the most common health problem.13 However, Mallick and Roldan Rojas surveyed 274 households in Bagerhat and observed that most respondents emphasized afflictions – such as arsenicosis, liver disease, respiratory ailments, and skin disease - unrelated to water-borne illnesses.35 Results from the present study emphasize the point implied empirically by this body of work and argued conceptually by Goff and Crow,36 that indicators narrowly focused on access to improved sources of drinking water will neglect other dimensions of the water scarcity burden. Even inclusion of metrics common in public health, such as diarrheal disease incidence, may be insufficient, as they neglect other ailments. Further, the variation in salinity observed suggests that future impact assessments should be designed with a range of relevant geographic and temporal scales.
This study is also one of the first to examine a spectrum of adaptation options and compare inhabitants’ preferences with available aid. The research team documented household- and community-level strategies, emphasized to varying degrees by participants (Table 2). As described in detail, the challenges highlighted by participants - especially community members - tended to be social and economic. Villagers emphasized barriers related to financial accessibility of RWH infrastructure, failure of NGO interventions to redress inaccessibility, skepticism about sharing arrangements, nepotism, and infrastructure siting. NGO representatives’ primary concerns included economic feasibility of providing aid, and community dynamics that facilitate/inhibit infrastructure maintenance. This research helps contextualize prior studies, particularly those that survey inhabitants’ adaptation preferences but provide limited insight into the obstacles faced in realizing them.13,37,38 It also helps put into perspective investigations that examine feasibility of interventions without incorporating inhabitants’ views. For example, to target poor households, Islam et al. designed a 2000-litre RWH tank using local materials and arrived at a cost of US$171, which they “assumed to be affordable in the region”.39 The present findings suggest that this assumption may not hold.
One study that did examine the process of adaptation from the perspective of affected inhabitants was conducted by Samaddar et al. in Bagerhat.40 However, their social network analysis of adopters of RWH tanks focused on how adopters may have been influenced to adopt tanks based on discussions with each other and observing neighboring households’ tank-owning behavior. Findings from the current study suggest that the main barrier for RWH is not awareness, but accessibility. Samaddar et al.'s analysis understates a key issue, which the socioeconomic profile of their participants reveals: tank adopters were far wealthier and more educated, working in non-agricultural occupations and earning on average US$180 monthly, while 40% of the municipality earned less than US$2 daily.
Among NGO stakeholders, the general argument is that it is not feasible or cost-effective to provide everyone with individual RWH infrastructure, and requiring households to contribute foments responsibility. From inhabitants’ perspective, the issues with the latter argument are that the required contributions or terms of assistance (eg, loans, samity membership) are still excessively burdensome, and that even when they are not prohibitive only a few politically well-connected households are selected as beneficiaries. With respect to the first argument, there are grounds to question the assumption that community-level infrastructure is truly more cost-effective, given that it often falls into disrepair. Many villagers claim they would take greater care of something individually owned.
The challenges with sustaining community-level interventions acknowledged by many NGO stakeholders in this study have also been confirmed by prior studies. For example, in Bagerhat and Khulna, Islam et al. found that most PSF taps were defective, while the size of community-level tanks prevented them from being washed even annually.41 Sultana et al. studied a community MAR-type system and reported significant time and costs for upkeep of the system (ie, extensive and frequent cleanings).42 At the same time, state actors reportedly have been reluctant to assume responsibility for maintaining this type of infrastructure. It is worth highlighting, in contrast, that water is recognized as both an economic and social good in Bangladesh and the National Water Policy recognizes access to water as a human right; however, no institution exists to manage water rights or protect human rights related to accessing water.43
Finally, it bears mention that much of the prior research has focused, not on the social and economic aspects of adaptation strategies, but rather on their technical aspects. Specifically, various studies based in the same districts have examined microbiological and physicochemical parameters to assess quality of water from RWH systems, unfiltered ponds, and PSFs.41,44–47 The general conclusion is that water from all of these options is unsafe for drinking due to coliform bacteria and E. coli, among other contaminants. PSF systems are not reliable in removing bacteria from pondwater, and one study found an increase in contaminants after filtration.41 RWH – at both community and household levels – yields water unsafe for drinking.41,44,47
Comparing these concerning assessments to practices and perspectives among this study’s participants, a disconnect is noted: first, although participants were dissatisfied with the quality of pondwater, they generally perceived rainwater to be ‘pure’; second, they mostly associated polluted rainwater with rainwater stored in maith, not in RWH tanks; third, physicochemical properties (eg, iron, salinity) and visible pollutants (debris, insects, etc.) were more concerning than microbiological contaminants; and fourth, home water treatment was far from universal, and the most commonly referenced method – alum, an (imperfect) disinfectant48,49 – was only applied to pondwater, if at all, for addressing turbidity. The current study expands in greater detail on prior research, which hints at a disconnect between drinking water assessments and community perspectives/practices.8,44,45 One takeaway is that although assessments have revealed that existing adaptation options yield water of poor quality, inhabitants of salinity-affected areas do not appear to share, or at least focus, on such concerns. Interventions on water quality may require additional efforts to sensitize targeted beneficiaries as to why they are necessary. Meanwhile, further investigations on how to make freshwater adaptation strategies accessible to all should be conducted to complement the existing, more technical body of research.
Limitations
Scholars have argued for the multi-scalar study of water governance, which envisions analysis across multiple scales – social, ecological, and spatial.50 Here, to achieve greater depth in understanding participants’ perspectives, this study was limited to a small spatial scale and leaves governance across larger scales (the Ganges basin, for example) for future research. Moreover, only rural domestic water use is addressed. A multi-scalar study of other usage domains – irrigation, mining and industry, and urban water supply – is pending.
Finally, in balancing with the intensive, qualitative focus of this study, salinity testing was constrained to two times and a smaller number of samples. Moreover, given the expertise of the team, researchers only tested salinity, leaving out other water quality parameters, which would have allowed a fuller characterization of freshwater availability. However, the salinity measurements help emphasize the situation of vulnerability and draw attention to the spatial and seasonal variability of the phenomenon.
CONCLUSIONS
Contributing to the literature on salinity, this research highlighted southwest Bangladesh as a case study of the serious, multifaceted impacts exerted by salinity on freshwater. The study has illuminated a key task ahead – to develop improved metrics that can adequately capture vulnerability to water insecurity in a changing environment. Moreover, notwithstanding interventions undertaken by development actors, there are still many gaps between the aid that is offered and the help that is required by those affected by salinity. Across the study areas, NGOs’ and inhabitants’ continuing concerns largely pertain to the social and economic aspects of adaptation. There is therefore a need, not only for increased technical, environmental health, and biomedical research to improve issues like water quality, but also for social science research to illuminate solutions for problems of accessibility, collective action, and accountability.
Acknowledgements
We thank the study participants for their time and insights, the research team (Afsana Sharmin, Abdul Matin, Dostogir Harun, and Leanne Unicomb) at the International Centre for Diarrhoeal Disease Research, Bangladesh for their invaluable participation in data collection and analysis, and Professors Robert Lawrence and William Ball at Johns Hopkins University for lending their expertise to this research.
Funding
This work was supported by the Johns Hopkins Center for a Livable Future-Lerner Fellowship, the Johns Hopkins Environment, Energy, Sustainability & Health Institute, and the Johns Hopkins Center for Qualitative Studies in Health and Medicine.
Competing interests
The authors have completed the Unified Competing Interest form at http://www.icmje.org/coi_disclosure.pdf (available on request from the corresponding author) and declare no conflict of interest.
Correspondence to:
Yukyan Lam
53 Knob Hill Road
Morganville NJ 07751
United States of America
[email protected]