A brief history of antibiotics
In 1928 Alexander Fleming identified penicillin, the world’s first antibiotic. Howard Florey and Ernst Chain later developed penicillin further so that it could be produced on a mass-scale, saving countless lives during World War II. Fleming, Chain and Florey were awarded the Nobel Prize for Medicine in 1945.
Antibiotics have undoubtedly revolutionised modern medicine. A US study in 1999 calculated that the introduction of antibiotics in 1936 caused deaths in the US to fall by 220 per 100,000 within 15 years. All other medical technologies combined over the next 45 years reduced deaths by only 20 per 100,000 people.1
Despite their benefits, we are finally realising that antibiotics are not infallible, and do more harm than good if misused.
Awareness of the dangers of misuse of antibiotics is not new; Fleming and his colleague, Almroth Wright, both cautioned the use of antibiotics several decades ago. At that time, Fleming highlighted that penicillin should only be used if indicated by an appropriate clinical diagnosis, and when used, the dose should be adequate, and the course should be completed fully.
Although the infamous quote “It is time to close the book on infectious diseases, and declare the war against pestilence won” was wrongly attributed to the US Surgeon General, Dr Stewart,2 many of his contemporaries held this belief, perpetuating a blasé attitude towards the use of antibiotics.
Thanks to antibiotic misuse, a lack of successful development of new antibiotics, and ever-increasing antibiotic resistance, we are now facing a real threat to the future of global healthcare.
What are antibiotics used for?
In addition to treating bacterial infections, antibiotics are used to guard against infections. Antibiotics make surgical operations possible, enable the survival of pre-term babies, and allow immuno-suppressant therapy (during chemo- or radiotherapy for cancer, or following organ transplant, for example).
With an ageing and increasingly unhealthy global population, chronic illnesses treated surgically (e.g. hip replacements) will become unsafe if we have no effective antibiotics.
How does antibiotic resistance develop?
Some bacteria are naturally resistant to certain types of antibiotics. However, bacteria may also become resistant: by a genetic mutation, or by one species acquiring resistance from another.
Genetic mutations can offer resistance in a number of ways, well described in a Nature review article3:
-
Mutations may enable the bacteria to produce enzymes to inactivate the antibiotics, either by hydrolysing the antibiotic, or by adding a chemical group to a vulnerable site of the drug. A well-known example of enzymatic inactivation is by β-lactamase, produced by bacteria to inactivate penicillins. Clavulanic acid, a β-lactamase inhibitor, is given in combination with penicillins to overcome this resistance;
-
Mutations may eliminate or alter the cell target that the antibiotic attacks;
-
Mutations may reduce permeability to antibiotics, by the downregulation of porins or by the replacement of porins with highly-selective channels;
-
Mutations may enable efflux pumps that export the antibiotic back outside.
Bacteria can acquire antibiotic resistance genes from other bacteria in several ways. Conjugation allows transfer of genes encoding resistance to antibiotics (found on plasmids and transposons) from one bacterium to another. Viruses can also pass mutations on. Bacteria also have the ability to acquire naked, “free” DNA from their environment.
Antibiotics exert a Darwinian selective pressure on bacteria. Susceptible bacteria are killed or inhibited by the antibiotic, whilst those with resistance survive and thrive. One of the main underlying problems is that many of the antibiotics we use today are ‘broad spectrum’ – they indiscriminately kill both the disease-causing bacteria and the healthy gut bacteria important to health. Resistant bacteria can flourish.
Bacteria can collect multiple resistance traits over time, and can therefore become resistant to many classes of antibiotics, or ‘multi-drug resistant’ (MDR). Bacteria that are MDR are colloquially termed ‘superbugs’.
How does antibiotic resistance spread?
Antibiotic resistance can spread ‘horizontally’, where bacteria share or exchange sections of genetic material with other bacteria, or ‘vertically’, where antibiotic resistance genes are passed on from one generation to the next.
Environmentally, antibiotic resistance spreads as the bacteria themselves move. Bacteria can travel in water, on food, and on or in people. People can pass the resistant bacteria to others, for example, by coughing or by contact with unwashed hands.
Why is resistance becoming an increasing problem?
As discussed, resistance can develop spontaneously or be acquired. Inappropriate use of antibiotics fosters the development of resistance. Antibiotics can be inappropriately used in the medical or veterinary setting.
In the healthcare world, doctors can face pressure from patients who believe antibiotics work on viruses. This is confounded by the fact that the term antibiotics is often used synonymously with antimicrobial, leading to the widespread but mistaken belief that antibiotics are effective against viral infections. In a European study, over half of French respondents expected an antibiotic for a flu-like illness.4
With a lack of ability to accurately diagnose bacterial from viral infections, or to quickly specify the bacteria and its susceptibility to antibiotics, doctors may prescribe an unnecessary antibiotic, or prescribe the wrong antibiotic.
Some healthcare systems effectively encouraged over prescription until recent times. In China, until 2010, doctors’ pay was based on profits from the sale of prescription drugs. One study found that almost every (98%) patient in one of the capital’s children’s hospital was given antibiotics for the common cold.5
In some countries, antibiotics can be purchased over-the-counter, or on-line. In India, for example, pharmacy sales of last-line antibiotics increased nearly sixfold between 2005-10.6
Outwith the medical setting, antibiotics are still overused around the world in livestock and fish farming. The European Commission banned the use of antibiotics as growth promoters in animal feed in the European Union, effective since the start of 2006,7 but the problem remains in some parts of the world. Resistant bacteria can be transferred to humans through direct contact with livestock and through the foodchain.
Resistance can also be spread from pollution from both farming and healthcare (from hospitals or from pharmaceutical plants) practices.
Why are there no new antibiotics?
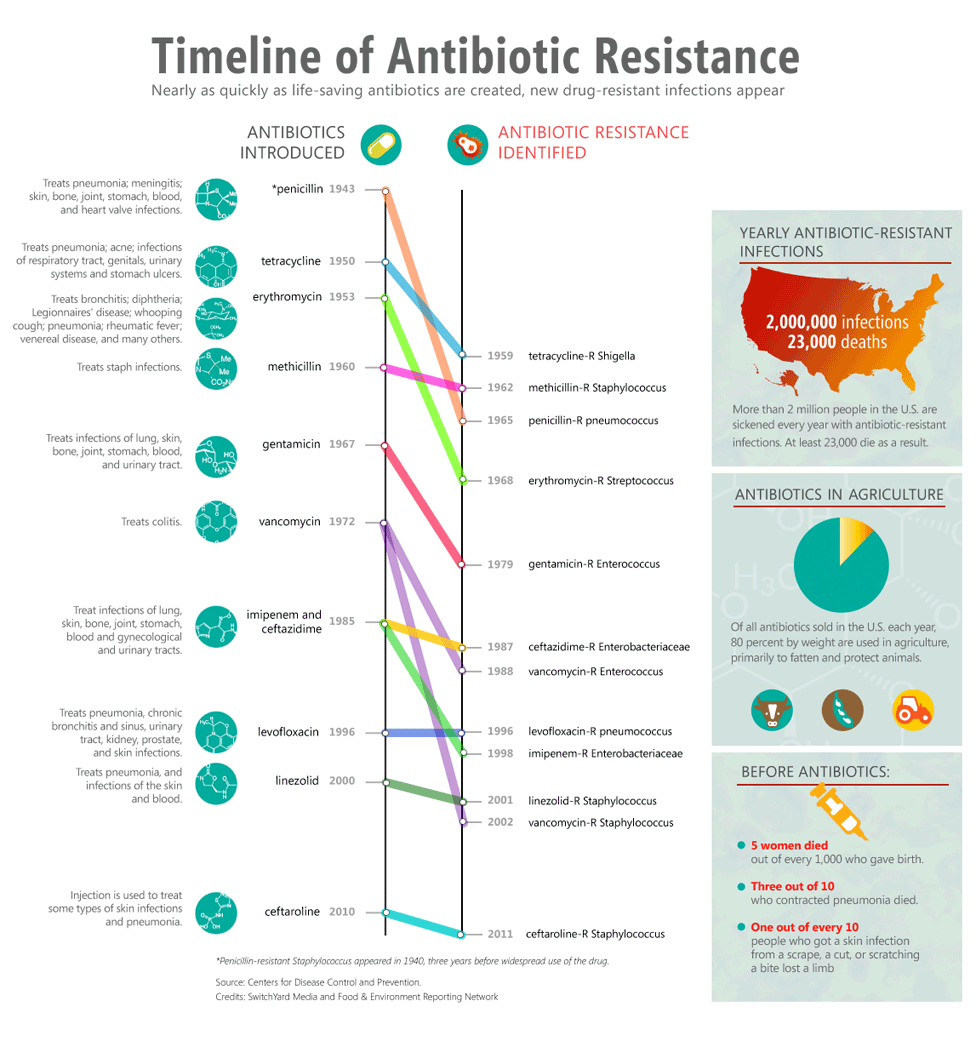
Figure 1, an infographic from the US-based Food & Environment Reporting Network, depicts a timeline of the introduction of antibiotics, and the years in which resistance to these were first observed.

There have effectively been no new classes of antibiotics discovered since 1987.8,9
There are a number of reasons for a lack of new antibiotics. Pivotally, antibiotics are not as profitable as other drugs. For example, drugs for chronic illnesses such as diabetes and hypertension offer a greater return on investment. Resistance is not an issue with these drugs, and these drugs will be used by many, many people, for many years. Any new antibiotics would likely be saved as a last-resort treatment, with only a short prescription length.
Respondents to the Global Risks Perception Survey connected antibiotic resistance to failure of the international intellectual property regime. This highlights a global market failure to promote antibiotic development through the promise of financial reward. This failure also undermines malarial drug development.10
How bad is the problem?
Very.
The world has only recently sat up and taken note of the impending dangers of antibiotic resistance.
About 25,000 patients a year die in the European Union from an infection caused by a bacteria that is resistant to more than one antibiotic – and on current trends this is predicted to grow to 390,000 a year by 2050.1
In 2014, David Cameron, the UK Prime Minister, echoed the thoughts of many world leaders and scientists when he said that a failure of action now will lead to an “almost unthinkable scenario where antibiotics no longer work and we are cast back into the dark ages of medicine”.9
Also in 2014, the World Health Organization (WHO) highlighted that antimicrobial resistance is a “serious threat [that] is no longer a prediction for the future, it is happening right now in every region of the world and has the potential to affect anyone, of any age, in any country”.11
The first report from the Review on Antimicrobial Resistance, “Antimicrobial Resistance: Tackling a Crisis for the Health and Wealth of Nations”, highlighted the macroeconomic impact on the world if no action is taken.12 This report estimated that failing to tackle drug resistance would cause 10 million extra deaths a year across the world by 2050. The reduction in population and the morbidity impact would also reduce the level of world GDP by 100 trillion USD by 2050.
In 2015, the WHO highlighted the main problems with resistance13:
-
Antibiotic resistance kills;
-
Antibiotic resistance hampers the control of infectious diseases: as people remain infectious for longer;
-
Antibiotic resistance is expensive: second- and third-line antibiotics are more expensive, and a longer stay in hospital means increased healthcare costs, and increased societal costs due to absence from work or education. The annual cost to the US health care system of antibiotic-resistant infections is already estimated at between 21-34 billion USD14;
-
Antibiotic resistance jeopardises healthcare gains to society: we need antibiotics to both treat and prevent infections.
In 2009, researchers found that none of the antibiotics in development would be effective against Klebsiella pneumoniae, which has become resistant to our strongest antibiotics (carbapenems), bringing with this resistance fatality rates of up to 50%.15
A recent Chinese study is very worrisome.16 Resistance to last-line antibiotics, polymyxins, has been observed. Although currently confined to China, the resistance is plasmid-mediated. The plasmid is a swappable circle of DNA that can easily be transferred - like other plasmid-borne resistance genes, this one is likely to go global.17
Antibiotic resistance is a particular problem in hospitals and in places like care homes, where many vulnerable people are gathered together in close proximity. Increased international travel is also problematic, because resistant bacteria can quickly and easily be spread globally. The consequences of a pandemic spread of antibiotic-resistant bacteria could include food shortages due to untreatable infections in livestock, and restrictions on trade in foodstuffs, and even on travel and migration.
What can we do?
We can work towards finding new treatments for bacterial infections. This falls into new antibiotics, and alternatives to antibiotics.
Although antibiotic development has been remarkably stagnant for decades, there is some hope. In early 2015, scientists reported the discovery of a new antibiotic, teixobactin, in a screen of uncultured bacteria.18 This novel antibiotic inhibits cell wall synthesis, and may therefore be less likely to promote resistance in Gram-positive bacteria, whose cell wall would likely always be vulnerable to this mechanism of action.
Additionally, there may be a new approach to antibiotic development based on bacteriocins, which are narrow-spectrum, protein antibiotics produced by bacteria to kill closely-related species.1
On the other hand, alternatives to antibiotics could be found. Newcastle University’s ALTAR trial (ALternatives To prophylactic Antibiotics for the treatment of Recurrent urinary tract infection in women) will compare a urinary antiseptic against the current standard of daily low-dose antibiotic.19 The hope is that this drug will be as effective, with fewer side effects and an almost non-existent chance of resistance development.
Despite these promising developments, if we continue to misuse and abuse drugs, the threat of resistance will never go away.
To really stand a chance of fighting antibiotic resistance, we need to work together, globally. A One Health approach, whereby veterinary and medical practitioners and researchers are united, will be needed.
Awareness is a key issue.
At the time of writing, the World Antibiotic Awareness Week was underway (16th-22nd November), which incorporated European Antibiotic Awareness Day (18th November). As part of this, the public, and animal and human healthcare communities were targeted to become an Antibiotic Guardian. Public Health England (PHE) established the Antibiotic Guardian campaign to help protect antibiotics and improve knowledge of antibiotic resistance. Guardianship involved taking a pledge to improve your own practice, and to discourage bad practice in others.
The Antibiotic Guardian campaign supports the UK 5 Year Antimicrobial Resistance Strategy 2013-18, established to slow the development and spread of antimicrobial resistance.
To educate patients, Treat Yourself Better has been established, detailing the symptoms of the cold and flu, and what people can do to manage these self-limiting illnesses themselves.20
Alongside its medical counterparts, the British Veterinary Association (BVA) is working hard to try to curtail inappropriate antibiotic use.21
Although much of the above relates to the United Kingdom, antibiotic resistance is a global issue as already emphasised, and must be tackled by the global community.
Perhaps no-one puts this better than Ramanan Laxminarayan. His TED talk22 is well worth a watch, and, with others, he has highlighted the need for global solutions to antibiotic resistance.23
In 2014, the World Health Organization gave its first global report on antibiotic resistance. They had a number of recommendations11:
-
Patients can help tackle resistance by using antibiotics as prescribed, and never sharing antibiotics with others;
-
Healthcare staff can help tackle resistance by improving infection prevention and control, and appropriate antibiotic prescription (the right antibiotic to the right people);
-
Policymakers can help tackle resistance by improving the monitoring of resistance, and regulate the appropriate use of antibiotics;
-
Policymaker and industry can help tackle resistance by fostering innovation, research and development of new treatments, and promoting cooperation amongst stakeholders.
In 2015, the WHO added to this,13 highlighting that people can help tackle resistance by hand washing, avoiding contact with sick people, using barrier contraception, and getting vaccinated.
The WHO works with the World Organisation for Animal Health (OIE) and the Food and Agriculture Organization of the United Nations (FAO) to promote best practices to avoid the emergence and spread of antibacterial resistance.
Furthermore, safe food handling and preparation is important in stopping the spread of bacteria, including resistant strains.
As is becoming more and more apparent, reducing meat consumption is an important global health goal. As antibiotics remain overused around the world in farming, reducing meat consumption should reduce the use of antibiotics globally. Furthermore, reducing meat consumption, especially red meat, has other global health benefits. Meat production is associated with global warming,24 and the WHO recently highlighted that processed meat, and possibly red meat, are carcinogenic.25
Antibiotic resistance is a global threat. We need to act now.
Funding
None.
Authorship declaration
CJG is the sole author.
Competing interests
The author completed the Unified Competing Interest form at www.icmje.org/coi_disclosure.pdf (available upon request from the corresponding author), and declares no conflict of interest.